Nasal polyps
Jump to navigation
Jump to search
The printable version is no longer supported and may have rendering errors. Please update your browser bookmarks and please use the default browser print function instead.
Nasal polyps are a common head and neck lesion. They are typically benign but may be malignant.
Overview
DDx (benign - multiple):[1]
- Autoimmune/idiopathic:
- Asthma.
- Allergic rhinitis.
- Churg-Strauss syndrome (AKA allergic granulomatous angiitis).
- Features: asthma, eosinophilia, granulomatous inflammation, necrotizing systemic vasculitis, and necrotizing glomerulonephritis.[2]
- Nonallergic rhinitis with eosinophilia syndrome (NARES).
- Infectious:
- Fungal infection (with allergic component - AFS = allergic fungal sinusitis).
- Chronic rhinosinusitis.
- Genetic:
- Primary ciliary dyskinesia.
- Cystic fibrosis.
- Associations:
- Alcohol intolerance ~ 50%.
- Aspirin intolerance - upto ~ 25%.
- Tumours:
- Juvenile nasopharyngeal angiofibroma - young males.
- Nasopharyngeal carcinomas.
- Sarcomas.
- Hemangioma.
- Schneiderian papilloma.
- Other.
Memory devices:
- GAIT = Genetic, Allergic/idiopathic, Infectious, Tumours.
- Allergic causes As - allergic, asthma, allergic granulomatous angiitis (Churg-Strauss syndrome), nonallergic rhinitis with eosinophilia.
Epidemiology
- More commonly assoc. with nonallergic conditions.[1]
Treatment
- Recurrent polyps: functional endoscopic sinus surgery (FESS).
Inflammatory polyps with neutrophils
General
- Histologic findings are non-specific; DDx includes:[3]
- Cystic fibrosis.
- Primary ciliary dyskinesia syndrome.
- Young syndrome
Microscopic
Features:
- Neutrophil predominant.
- Edema.
- +/-Mucus-impaction (dilated glands with mucus).
- Suggestive of cystic fibrosis.[4]
Sign out
A. Nasal sinus tissue, right, excision: - Inflamed edematous sinonasal mucosa with abundant neutrophils. - Negative for malignancy. B. Nasal sinus tissue, left, excision: - Inflamed edematous sinonasal mucosa with abundant neutrophils and fragments of bone. - Negative for malignancy.
Alternate
A. Contents of Left Ethmoid Sinus, Excision:
- Mildly inflamed sinonasal mucosa with bone and fibrous tissue.
- NEGATIVE for malignancy.
B. Contents of Right Ethmoid Sinus, Excision:
- Mildly inflamed sinonasal mucosa with bone and fibrous tissue.
- NEGATIVE for malignancy.
Allergic nasal polyp
General
- People with allergies.
- Same type of polyps seen in those without allergies.[5]
Gross
- Polypoid mass - several millimetres to centimetres in size.
- Translucent.[citation needed]
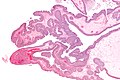
Microscopic
Features:[6]
- Normal respiratory epithelium.
- Stroma with:
- Edema.
- Eosinophils.
- +/-Other inflammatory cells (plasma cells, lymphocytes, neutrophils).
DDx:
- Inflammatory nasal polyp with abundant neutrophils.
- Vasculitis.
- Biphenotypic sinonasal sarcoma - has hypercellular stroma.
Sign out
A. Left Nasal Polyp, Excision: - Inflamed edematous sinonasal mucosa with abundant eosinophils. - NEGATIVE for malignancy. B. Right Nasal Polyp, Excision: - Inflamed edematous sinonasal mucosa with abundant eosinophils and fragments of bone. - NEGATIVE for malignancy.
A. Nasal sinus tissue, right, excision: - Inflamed edematous sinonasal mucosa with abundant eosinophils. - Negative for malignancy. B. Nasal sinus tissue, left, excision: - Inflamed edematous sinonasal mucosa with abundant eosinophils and fragments of bone. - Negative for malignancy.
Block letters
A. NASAL SINUS TISSUE, RIGHT, EXCISION: - INFLAMED EDEMATOUS SINONASAL MUCOSA WITH ABUNDANT EOSINOPHILS. - NEGATIVE FOR MALIGNANCY. B. NASAL SINUS TISSUE, LEFT, EXCISION: - INFLAMED EDEMATOUS SINONASAL MUCOSA WITH ABUNDANT EOSINOPHILS AND FRAGMENTS OF BONE. - NEGATIVE FOR MALIGNANCY.
Schneiderian papilloma
General
- Lumpers vs. splitters debate about whether it is one entity or three.[8]
- Inverted (Schneiderian) - most common ~60-65%.
- Fungiform (Schneiderian) - less common ~30-35%.
- Oncocytic (Schneiderian) - least common ~5%.
Inverted
- AKA inverted papilloma.[9]
- Usually lateral wall (as the septum as little soft tissue to grow into).[8]
- May transform to carcinoma.
Fungiform
Oncocytic
Microscopic
Inverted Schneiderian papilloma
Features:[8]
- Well-demarcated epithelial islands in the stroma.
- Squamous +/-surface keratinization or respiratory type epithelium (with cilia).
- +/-Neutrophils.
- +/-Goblet cells.
Notes:
- May mimic invasive SCC.
Images
Schneiderian papilloma - very low mag. (WC)

Schneiderian papilloma - very high mag. (WC)


Fungiform Schneiderian papilloma
Features:
- Exophytic growth pattern - key feature.
Oncocytic Schneiderian papilloma
Features:
- Oncocytes - key feature.
- Exophytic or endophytic growth pattern.
Antrochoanal polyp
- Abbreviated ACP.
General
Epidemiology:
- "Almost always" recur if incompletely excised.[12]
- Originates from maxillary sinus and extends to choana.[13]
Microscopic
Features:[14]
- Respiratory epithelium.
- Relatively pauciglandular - when compared to inflammatory nasal polyps.
- Typically few eosinophils.
DDx:
- Inflammatory nasal polyps.
Sign out
Ethmoid Sinus Contents (Right), Excision:
- Benign nasal polyp (antrochoanal type) and mildly inflamed sinonasal mucosa.
- NEGATIVE for malignancy.
See also
References
- ↑ 1.0 1.1 URL: http://emedicine.medscape.com/article/994274-overview. Accessed on: 16 March 2011.
- ↑ http://emedicine.medscape.com/article/333492-overview
- ↑ URL: http://emedicine.medscape.com/article/994274-diagnosis. Accessed on: 16 March 2011.
- ↑ Beju D, Meek WD, Kramer JC (April 2004). "The ultrastructure of the nasal polyps in patients with and without cystic fibrosis". J. Submicrosc. Cytol. Pathol. 36 (2): 155–65. PMID 15554502.
- ↑ Davidsson, A.; Hellquist, HB. (1993). "The so-called 'allergic' nasal polyp.". ORL J Otorhinolaryngol Relat Spec 55 (1): 30-5. PMID 8441521.
- ↑ Klatt, Edward C. (2006). Robbins and Cotran Atlas of Pathology (1st ed.). Saunders. pp. 144. ISBN 978-1416002741.
- ↑ URL: http://emedicine.medscape.com/article/862677-overview. Accessed on: 19 November 2011.
- ↑ 8.0 8.1 8.2 8.3 8.4 8.5 Barnes L (March 2002). "Schneiderian papillomas and nonsalivary glandular neoplasms of the head and neck". Mod. Pathol. 15 (3): 279–97. doi:10.1038/modpathol.3880524. PMID 11904343. http://www.nature.com/modpathol/journal/v15/n3/full/3880524a.html.
- ↑ Vrabec, DP. (May 1994). "The inverted Schneiderian papilloma: a 25-year study.". Laryngoscope 104 (5 Pt 1): 582-605. PMID 8189990.
- ↑ Bravo Domínguez, O.; Vela Cortina, M.; Ramírez Ruiz, RD.; Ros Vergara, A.; Dinarés Jaumeandreu, D.; Encina Ruiz, L.; Arias Cuchí, G.; Ardíaca Bosch, MC. et al. (2005). "[Oncocytic schneiderian papilloma. A case report].". An Otorrinolaringol Ibero Am 32 (2): 115-23. PMID 15929584.
- ↑ Maldonado M, Martínez A, Alobid I, Mullol J (December 2004). "The antrochoanal polyp". Rhinology 42 (4): 178–82. PMID 15626248.
- ↑ 12.0 12.1 Frosini P, Picarella G, De Campora E (February 2009). "Antrochoanal polyp: analysis of 200 cases". Acta Otorhinolaryngol Ital 29 (1): 21–6. PMC 2689564. PMID 19609378. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2689564/.
- ↑ Balikci HH, Ozkul MH, Uvacin O, Yasar H, Karakas M, Gurdal M (May 2013). "Antrochoanal polyposis: analysis of 34 cases". Eur Arch Otorhinolaryngol 270 (5): 1651–4. doi:10.1007/s00405-012-2274-2. PMID 23179936.
- ↑ Min YG, Chung JW, Shin JS, Chi JG (July 1995). "Histologic structure of antrochoanal polyps". Acta Otolaryngol 115 (4): 543–7. doi:10.3109/00016489509139364. PMID 7572133.