C-cell hyperplasia
Jump to navigation
Jump to search
The printable version is no longer supported and may have rendering errors. Please update your browser bookmarks and please use the default browser print function instead.
| C-cell hyperplasia | |
|---|---|
| Diagnosis in short | |
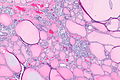
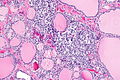
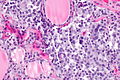
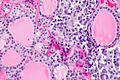
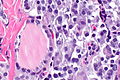
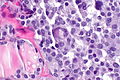
 C-cell hyperplasia. H&E stain. | |
| LM DDx | medullary thyroid carcinoma |
| IHC | CEA +ve, chromogranin A +ve, synaptophysin +ve |
| Gross | not apparent; mid portion of lobe to upper third of lobe |
| Site | thyroid gland |
|
| |
| Syndromes | Multiple endocrine neoplasia type 2A, Multiple endocrine neoplasia type 2B |
|
| |
| Clinical history | +/-family history of thyroid cancer or MEN 2A or MEN 2B |
| Signs | +/-marfanoid habitus (seen in MEN 2B) |
| Prevalence | uncommon |
| Blood work | calcitonin level elevated |
| Prognosis | benign in itself |
| Treatment | prophylatic surgery |
C-cell hyperplasia, abbreviated CCH, is a pathology of the thyroid gland and considered the precursor for medullary thyroid carcinoma.
General
- Screening for C-cell hyperplasia/medullary thyroid carcinoma done with serum calcitonin level.[1]
Associated with:
- Multiple endocrine neoplasia type 2A[2] - may be found in specimen of a surgery done to exclude MTC in the context of MEN 2A.[3]
- Multiple endocrine neoplasia type 2B.[4]
Gross
- Not visible on gross.
Location:[5]
- Mid portion of lobe to upper third of lobe.
- Not at the poles.
- Not in the isthmus.
Microscopic
Features:
- Definitions vary.[6]
- One definition - either of the following:[1]
- >50 C-cells per low-power field (x100).
- This part of the definition suffers from LPFitis.
- "Medullary thyroid carcinoma confined to the thyroid gland and no larger than 10 mm in greatest dimension."
- >50 C-cells per low-power field (x100).
- Another definition:
- Invasion of the basement membrane with stromal reaction.
- A third definition:
- "Several clusters" of more than six C cells.
- One definition - either of the following:[1]
Images
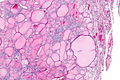
CCH in MEN - very low mag. (WC)
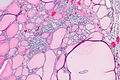
CCH in MEN - low mag. (WC)
CCH in MEN - low mag. (WC)
CCH in MEN - intermed. mag. (WC)
CCH in MEN - high mag. (WC)
CCH in MEN - high mag. (WC)
CCH in MEN - very high mag. (WC)
CCH in MEN - very high mag. (WC)








CCH in MEN - chromo A - intermed. mag. (WC)
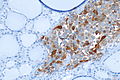
CCH in MEN - chromo A - high mag. (WC)

CCH in MEN - chromo A - very high mag. (WC)

CCH in MEN - CEA - low mag. (WC)
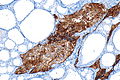
CCH in MEN - CEA - intermed. mag. (WC)

CCH in MEN - CEA - high mag. (WC)

CCH in MEN - CEA - very high mag. (WC)







www
- CCH - crappy B&W image (nature.com).[7]
- CCH - crappy B&W image (nature.com).
- CCH (forpath.org).[8]
- CCH (unibas.ch).
- Nodular CCH (unibas.ch).
{kind=link}
IHC
- Chromogranin A +ve.
- CEA +ve.
- Synaptophysin +ve.
See also
References
- ↑ 1.0 1.1 Machens A, Hoffmann F, Sekulla C, Dralle H (December 2009). "Importance of gender-specific calcitonin thresholds in screening for occult sporadic medullary thyroid cancer". Endocr. Relat. Cancer 16 (4): 1291–8. doi:10.1677/ERC-09-0136. PMID 19726541. http://erc.endocrinology-journals.org/cgi/content/full/16/4/1291.
- ↑ Tyer, NM.; Braunstein, GD.; Frishberg, D.. "Unusual case of multiple endocrine neoplasia type 2A syndrome without medullary thyroid carcinoma.". Endocr Pract 17 (2): e4-7. doi:10.4158/EP10157.CR. PMID 21134882.
- ↑ Etit, D.; Faquin, WC.; Gaz, R.; Randolph, G.; DeLellis, RA.; Pilch, BZ. (Nov 2008). "Histopathologic and clinical features of medullary microcarcinoma and C-cell hyperplasia in prophylactic thyroidectomies for medullary carcinoma: a study of 42 cases.". Arch Pathol Lab Med 132 (11): 1767-73. doi:10.1043/1543-2165-132.11.1767. PMID 18976013.
- ↑ Pagon, RA.; Adam, MP.; Ardinger, HH.; Wallace, SE.; Amemiya, A.; Bean, LJH.; Bird, TD.; Fong, CT. et al. Multiple Endocrine Neoplasia Type 2. PMID 20301434.
- ↑ URL: http://www.cap.org/apps/docs/committees/cancer/cancer_protocols/2011/Thyroid_11protocol.pdf. Accessed on: 7 April 2012.
- ↑ Raphael S. 17 January 2011.
- ↑ Guyétant, S.; Josselin, N.; Savagner, F.; Rohmer, V.; Michalak, S.; Saint-André, JP. (Aug 2003). "C-cell hyperplasia and medullary thyroid carcinoma: clinicopathological and genetic correlations in 66 consecutive patients.". Mod Pathol 16 (8): 756-63. doi:10.1097/01.MP.0000081727.75778.0C. PMID 12920219.
- ↑ URL: http://www.forpath.org/workshops/0201/html/case_7.asp. Accessed on: 21 May 2013.