Desmoid-type fibromatosis
| Desmoid-type fibromatosis | |
|---|---|
| Diagnosis in short | |
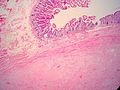
 Desmoid-type fibromatosis. H&E stain. | |
|
| |
| LM | "sweeping fascicles"/bundles, spindle cells with small slender nuclei, solid dark eosinophilic cytoplasm, +/-mitoses, long thin-walled vessels - parallel to one another |
| LM DDx | hypertrophic scar, gastrointestinal stromal tumour, retroperitoneal fibrosis, other fibromatoses, nodular fasciitis, schwannoma |
| IHC | beta-catenin +ve (nuclear), SMA +ve/-ve, CD117 -ve |
| Site | soft tissue |
|
| |
| Syndromes | familial adenomatous polyposis - esp. Gardner syndrome |
|
| |
| Prevalence | uncommon |
| Prognosis | benign but locally aggressive |
| Clin. DDx | trauma/hematoma |
Desmoid-type fibromatosis is a benign soft tissue lesion in the fibroblastic/myofibroblastic group of tumours.
It is also known as desmoid tumour and desmoid fibromatosis.
General
- Benign.
- One of many fibromatoses.
- Locally aggressive.[1]
- May be seen in the context of familial adenomatous polyposis.
Gross
Features:[2]
- Location:
- Abdominal wall, proximal extremities - classic for adolescents and women.
- Head and neck - classic for children.
- Circumscribed mass.
- May be quite large (>10 cm).
Microscopic
- "Sweeping fascicles"/bundles.
- Spindle cells with:
- Small slender nuclei.
- Solid dark eosinophilic cytoplasm.
- +/-Mitoses - may be abundant.
- Long thin-walled vessels - parallel to one another - important feature.
DDx:
- Hypertrophic scar-like lesion, see dermal scar.
- Gastrointestinal stromal tumour[4] - reported in abdominal wall.[5]
- Retroperitoneal fibrosis - no beta-catenin staining.[4]
- Other fibromatoses.
- Nodular fasciitis - esp. with RBC extravasation.
- Schwannoma.
- Solitary fibrous tumour - may be a consideration for a collagenous desmoid. Desmoids should lack staghorn vessels.
- Inflammatory fibroid polyp - may be a consideration for tumors invading into bowel wall.
Images

Desmoid tumour. (WC)
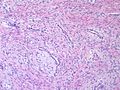
Classic desmoid fibromatosis with delicate curving vessels and sweeping long fascicles.
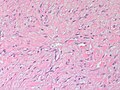
This example of desmoid fibromatosis shows a keloidal collagenous stroma and may evoke keloidal scar or even solitary fibrous tumor.
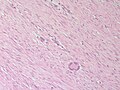
Giant cells are an unusual but occasional component of desmoid fibromatosis. Sometimes the giant cells are histiocytic, sometimes they are entrapped rhabdomyocytes.
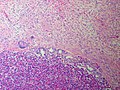
Intra-abdominal desmoids can overrun vital organs; in this case, the pancreas.
Intraabdominal desmoids can extend through the bowel to the mucosa and provoke ulceration.





www:
- Desmoid tumour (surgicalpathologyatlas.com).
- Desmoid tumour (cheapmedicinechest.com).[6]
- Desmoid tumour (radiographics.rsna.org).
- Desmoid-type fibromatosis (nih.gov).[7]
{kind=link}
IHC
Features:[2]
- Beta-catenin +ve (nuclear[4]) - important.
- 100% sensitive... may not be completely specific (?).[8]
- Staining may be difficult to interpret as the nucleus may be small, the cytoplasm scant and the precipitate grainy and vague. Ensure that the staining seen is nuclear (or nuclear and cytoplasmic). Cytoplasmic staining alone can occur and is not a true positive.
- SMA +ve ~50% of lesions.
Others:
- CD117 -ve.
- DOG1 -ve.
- CD34 -ve.
Sign out
LESION, ABDOMINAL WALL, BIOPSY: - DESMOID-TYPE FIBROMATOSIS. COMMENT: The tumour stains strongly with beta-catenin and weakly with SMA. It is negative for CD117.
See also
References
- ↑ URL: http://www.dtrf.org/dtrf_aboutdesmoids.htm. Accessed on: 15 April 2011.
- ↑ 2.0 2.1 2.2 Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 609. ISBN 978-0781765275.
- ↑ URL: http://www.surgicalpathologyatlas.com/glfusion/mediagallery/media.php?f=0&sort=0&s=20090717111548196. Accessed on: 4 October 2011.
- ↑ 4.0 4.1 4.2 Huss, S.; Nehles, J.; Binot, E.; Wardelmann, E.; Mittler, J.; Kleine, MA.; Künstlinger, H.; Hartmann, W. et al. (Jan 2013). "β-catenin (CTNNB1) mutations and clinicopathological features of mesenteric desmoid-type fibromatosis.". Histopathology 62 (2): 294-304. doi:10.1111/j.1365-2559.2012.04355.x. PMID 23020601.
- ↑ Thalheimer, A.; Meyer, D.; Gattenlöhner, S.; Timmermann, W.; Thiede, A. (Jul 2004). "[Gastrointestinal stromal tumor of the abdominal wall. An unusual localization of a rare tumor].". Chirurg 75 (7): 708-12. doi:10.1007/s00104-003-0696-5. PMID 15257404.
- ↑ URL: http://www.cheapmedicinechest.com/abdominal-pain-and-colonic-obstruction-from-an-intra-abdominal-desmoid-tumor.html. Accessed on: 4 October 2011.
- ↑ Ma, JH.; Ma, ZH.; Dong, XF.; Yin, H.; Zhao, YF. (Jun 2013). "Abdominal wall desmoid tumors: A case report.". Oncol Lett 5 (6): 1976-1978. doi:10.3892/ol.2013.1297. PMID 23833679.
- ↑ Amary, MF.; Pauwels, P.; Meulemans, E.; Roemen, GM.; Islam, L.; Idowu, B.; Bousdras, K.; Diss, TC. et al. (Sep 2007). "Detection of beta-catenin mutations in paraffin-embedded sporadic desmoid-type fibromatosis by mutation-specific restriction enzyme digestion (MSRED): an ancillary diagnostic tool.". Am J Surg Pathol 31 (9): 1299-309. doi:10.1097/PAS.0b013e31802f581a. PMID 17721184.