Hepatitis C
Hepatitis C is type of chronic viral hepatitis caused by the hepatitis C virus (abbreviated HCV).
It is a type of medical liver disease
General
- Leads to hepatocellular carcinoma in the setting of cirrhosis.
- Tends to be chronic; the "C" in "hepatitis C" stands for chronic.
- Diagnosis is by serology.
Associated pathology:
Microscopic
Features:
- Lobular inflammation - this is non-specific finding.
- Usually Grade 1, rarely Grade 2 and almost never Grade 3 or Grade 4.[1]
- Periportal steatosis in genotype 3.[2]
- Steatosis in hepatitis C is usually a secondary pathology, i.e. a separate pathologic process.[3]
Images
Acute hepatitis C Acute hepatitis C Acute hepatitis C Acute hepatitis C Acute hepatitis C
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Acute hepatitis C presenting in a 37 year old woman with a 3 week history of jaundice, normal hepatobiliary radiologic studies, bilirubin 11.2, alkaline phosphatase 257, alanine aminotransferase 594, albumin 3, normal complete blood count, normal platelet level. No medications. A. Low power shows inflammation of triads (black arrow) with interface change, as well as disordered lobule with inflammation (red arrow). B. The triads showed intense lymphohistiocytic inflammation with interface hepatitis. Note piecemeal necrosis (black arrow) and neutrophils (red arrows). C. The hepatocytes appear haphazardly arranged with chronic inflammatory cells surrounding them in abundance. The arrow points to a Councilman body. C. Reticulin showed only isolated cell piecemeal necrosis in a minority of triads (black arrow). Regenerative cords two-three nuclei thick (green arrow) were only rarely seen. Significant collapse was not seen. D. PAS-D highlighted bile ductular proliferation (arrows). E. Feathery degeneration (foamy macrophage-like hepatocytes) was prominent in some areas. [4]
A. 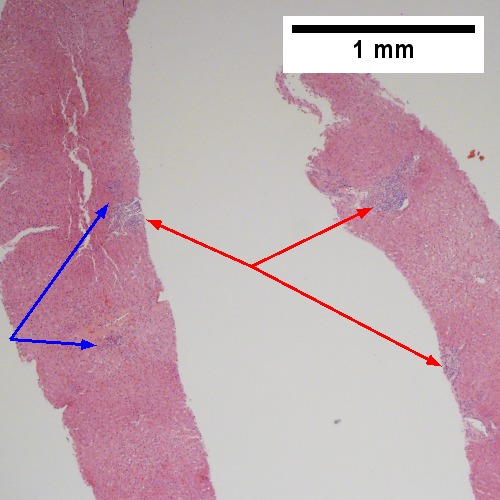
B. 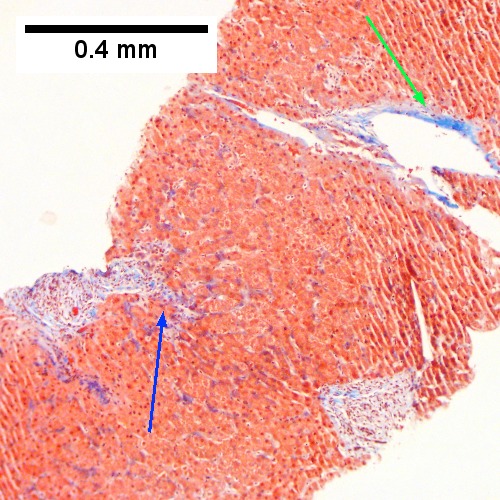
C. 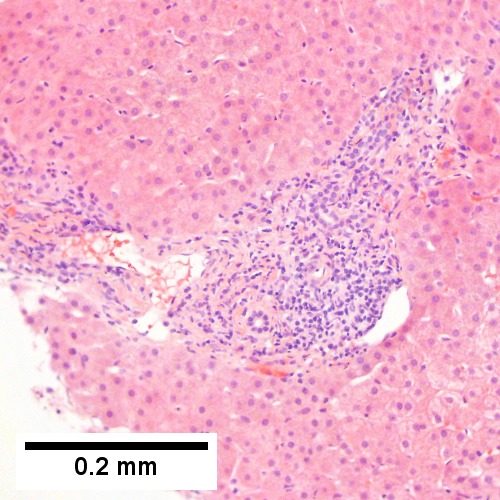
D. 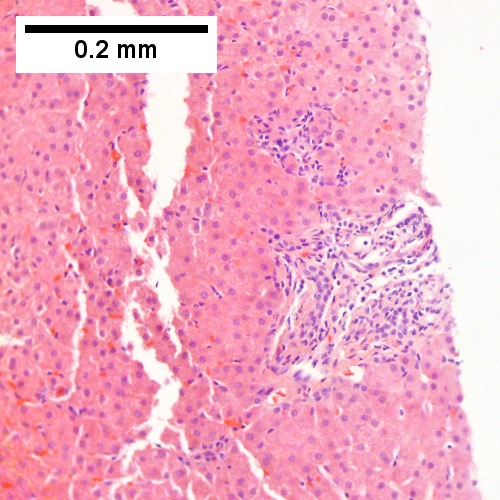
E. 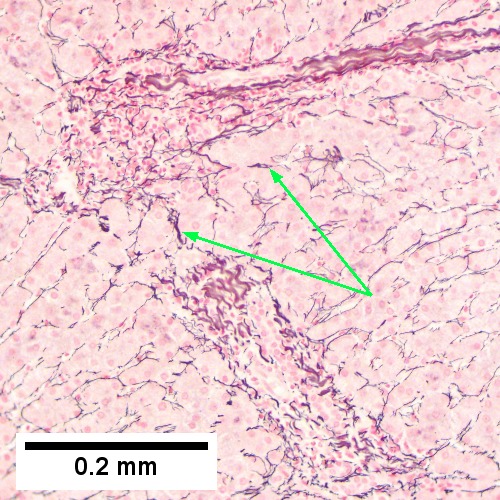
F. 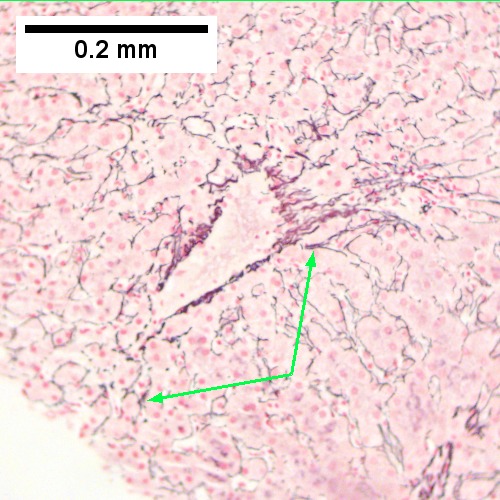
Hepatitis C virus. Metavir Activity Index 1 (PMN 0 LN 1). A. Preserved architecture shows small, inflamed triads [red arrows] and foci of spotty necrosis [blue arrows]. B. Trichrome shows periportal fibrosis [blue arrow] and central venous sclerosis [green arrow]. C. A higher power view of an inflamed triad with interface hepatitis, but a smooth outline, suggesting no piecemeal necrosis. D. A focus of spotty necrosis near an unafflicted triad below it. E. Reticulin shows collapse [arrows] extending from/near portal triad without piecemeal necrosis. F. Reticulin shows collapse [arrows] extending from/near central vein.
A. 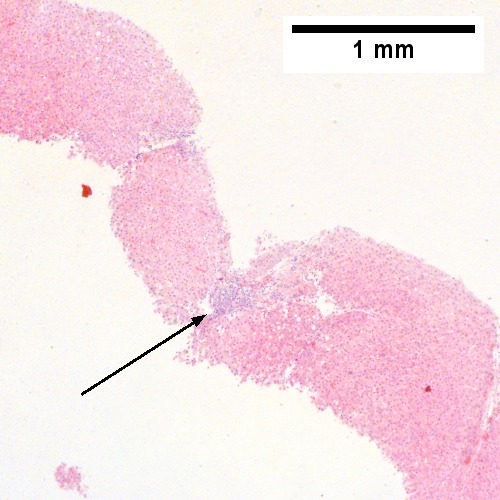
B. 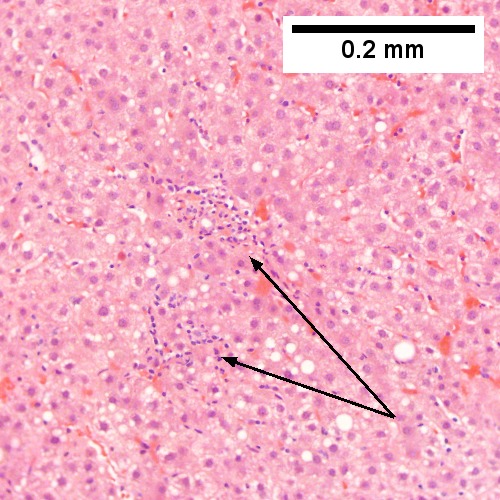
C. 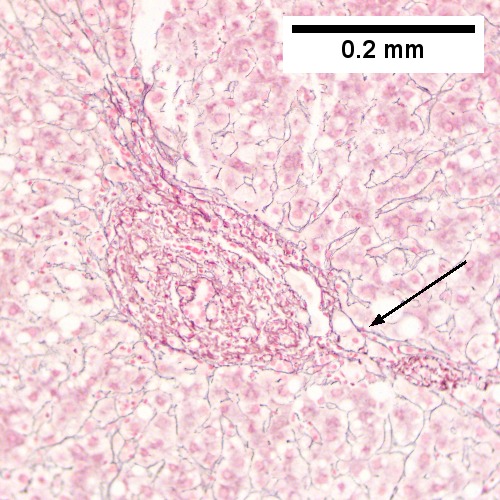
D. 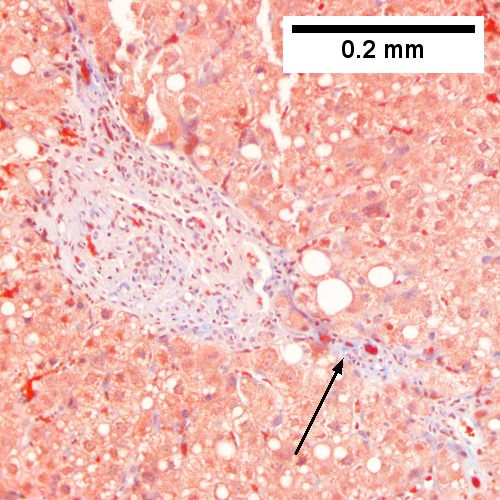
E. 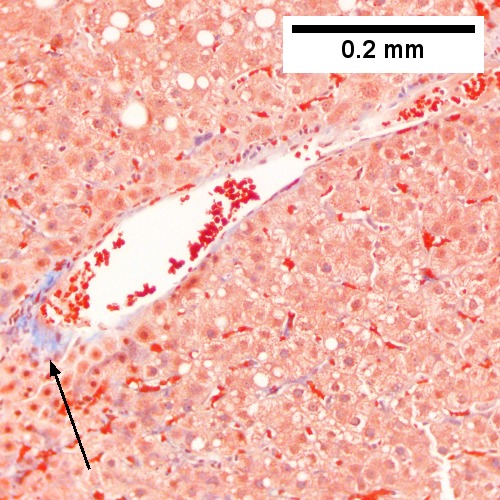
F. 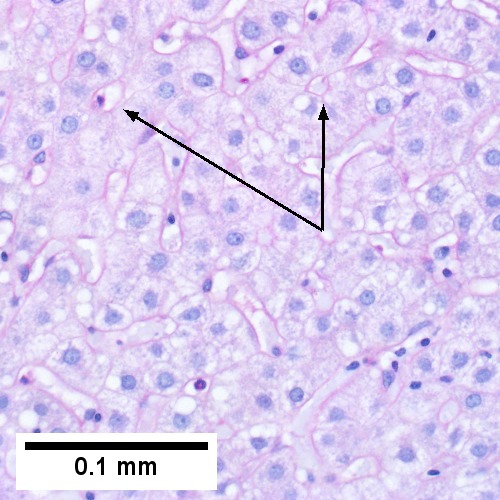
Hepatitis C virus. Metavir activity index 1 (PMN 1 LN 1). A. Triads show inflammation with extension to portal border (interface hepatitis). B. Lymphocyte aggregates denote spotty necrosis. C. Reticulin shows focal piecemeal necrosis [arrow]. D. Trichrome shows periportal fibrous extension [arrows]. E. Trichrome shows sclerosis of central vein. F. PAS D can be useful when steatosis frustrates rosette identification; hepatocyte rosettes [arrows] have red edges.
A. 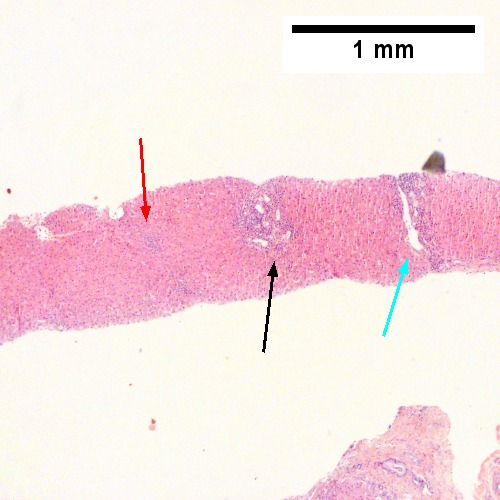
B. 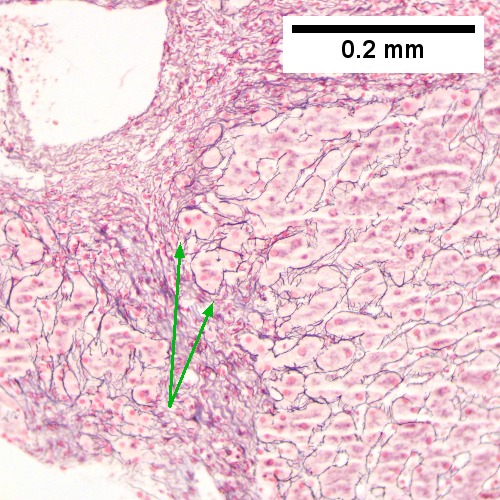
C. 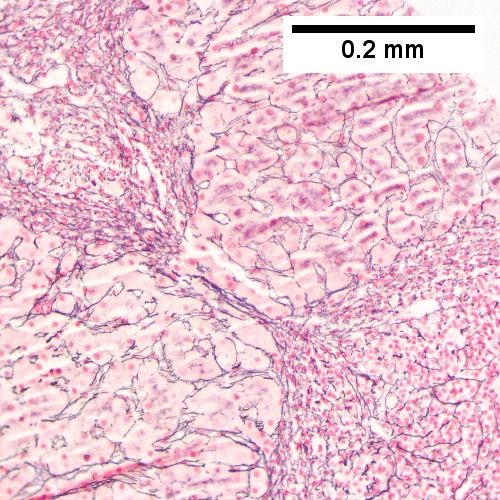
D. 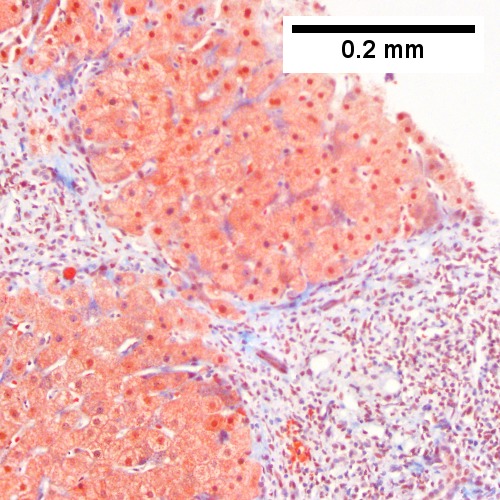
E. 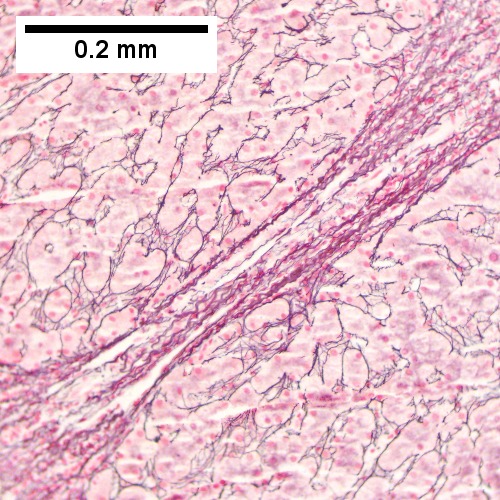 F.
F. 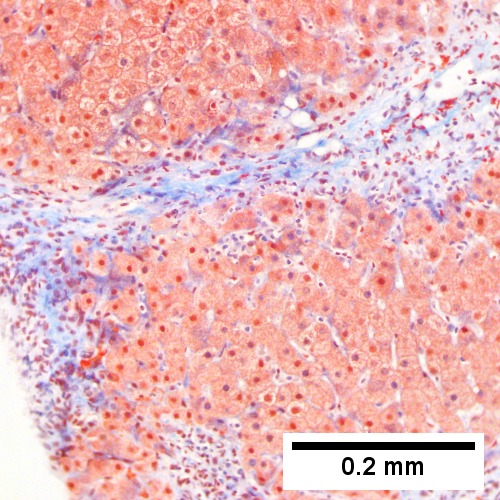
Hepatitis C Virus. Metavir Activity Index 2 (PMN 1 LN 2) Metavir fibrosis stage 3. A. Low power showing a focus of spotty necrosis [red arrow], a triad with inflammation bounding its edge (interface necrosis) [black arrow] and a bridge [cyan arrow]. B. Reticulin showing a focus of piecemeal necrosis [arrows], where black lines bound hepatocytes & hepatocyte clusters, not a continuous region. C. Reticulin showing collapse between triads, not a bridge, given cells within strands. D. Trichrome showing collapse between triads, not a bridge, given atrophic cells precluding continuous connection between triads; the fibrosis about the triads is, on each side, a mere spike set. E. Reticulin showing a bridge, given lack of definite hepatocyte type cells within strands. F. Trichrome showing a bridge, with collagenous continuity uninterrupted by hepatocytes.
A. 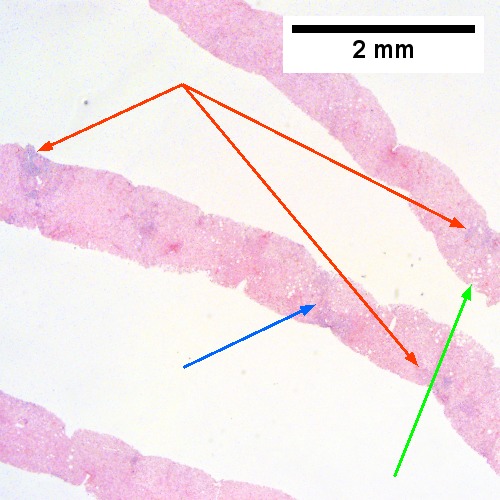
B. 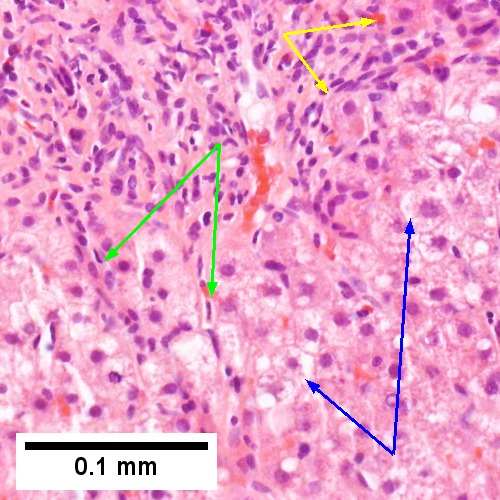
C. 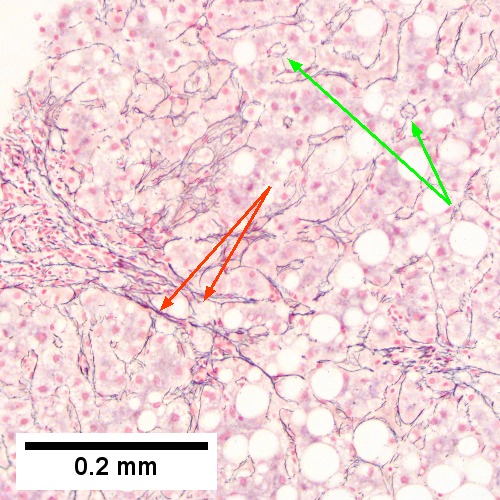
D. 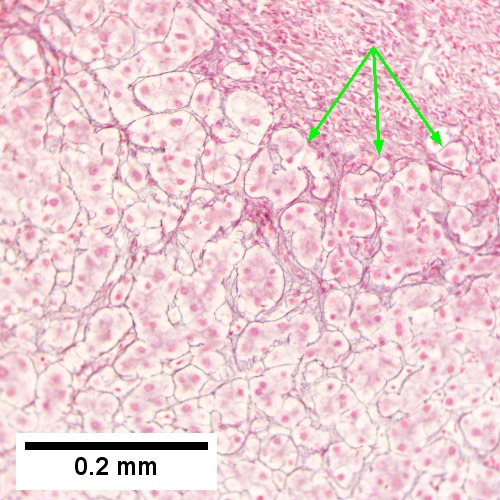
E. 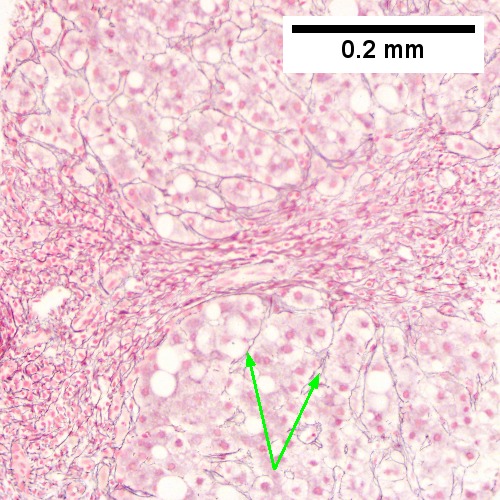
F. 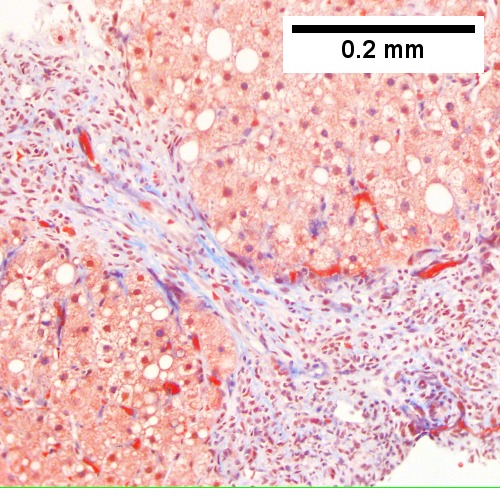
Hepatitis C. Metavir Activity Index 2 (PMN2, LN1), Metavir fibrosis stage 3. A.
Expanded dark triads, indicating interface hepatitis [red arrows], foci of steatosis [green arros], potential bridge [blue arrow]. B. Extending from triad are stretches of apparent necrosis [green arrows], inflammatory cells bound hepatocytes afflicted by piecemeal necrosis [yellow arrows], ballooning degeneration denoted by cytoplasmic tufts [blue arrows]. C. Reticulin shows collapse (necrosis) with thick bands [red arrows], as well as rosettes [green arrows] indicating dilated cholangioles. D. Reticulin here shows continuous piecemeal necrosis with black bounded hepatocyte islets [arrows]. E. Reticulin here shows a bridge with regeneration, wherein two or more nuclei lie between reticulin lines [arrows]. F. Trichrome demarcates one of the bridges (Row 3 Right 200X).
33.589444 101.891944
33.589444 101.891944
33.589444 101.891944
33.589444 101.891944
33.589444 101.891944
Hepatitis C virus. Metavir activity index 3. Metavir fibrosis stage 1. A. Two dark expanded triads (arrows) have fuzzy edges. B. A triad shows interface hepatitis by lymphocytes and macrophages, with surrounding of hepatocytes (black arrows), piecemeal necrosis, with collections in the lobule (green arrows), spotty necrosis. The portal triad, venule and artery (blue arrows) are unaffected. The central vein’s being near the triad with a small pink line (yellow arrows) indicates significant collapse. C. Reticulin. Thick black lines between triad and central vein (blue arrows) document significant necrosis (LN 2). Two-three cell thick cords (green arrows) show regeneration. D. Reticulin. Thick black lines extending from triad, but not to a central vein, (blue arrows) are not as significant. Black lines surrounding multiple hepatocytes (green arrows) indicate moderate piecemeal necrosis (PMN 2), not severe because it does not involve most of the triad of most triads. E. Trichrome. Only fibrosis of portal triads was seen, indicating metavir fibrosis stage 1.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A. 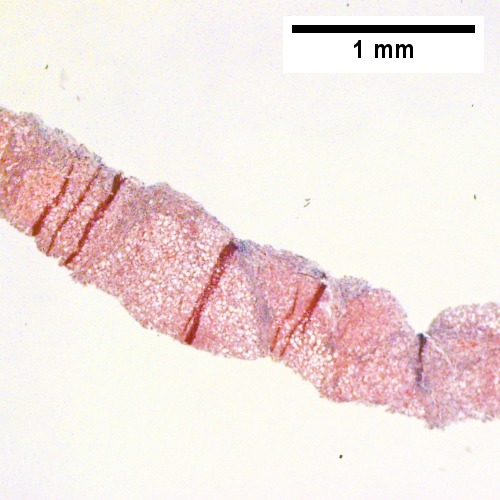
B. 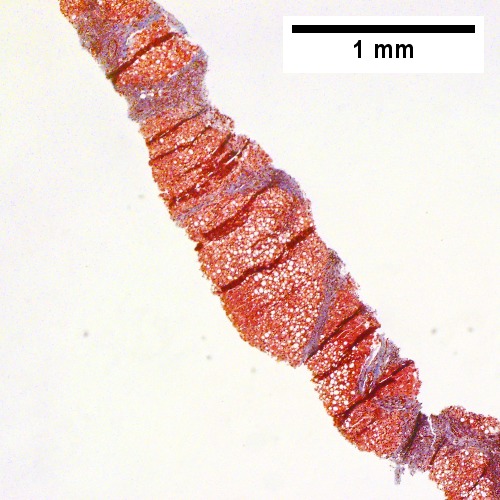
C. 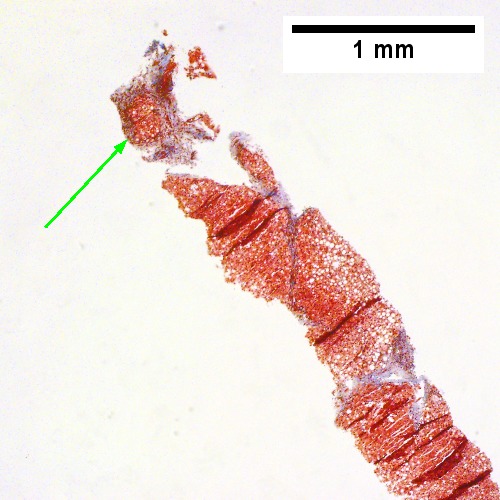
D. 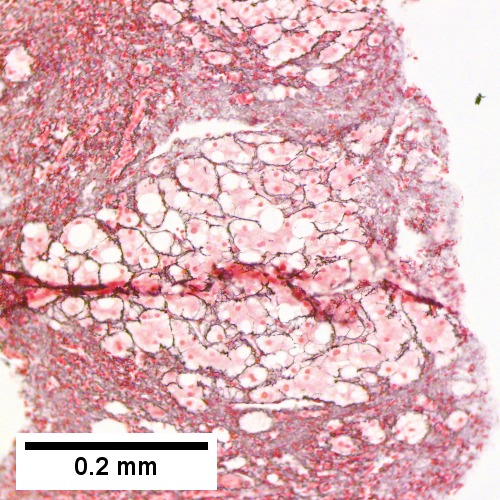
E. 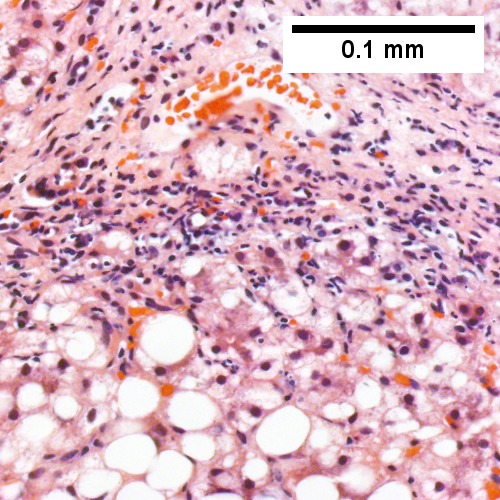
F. 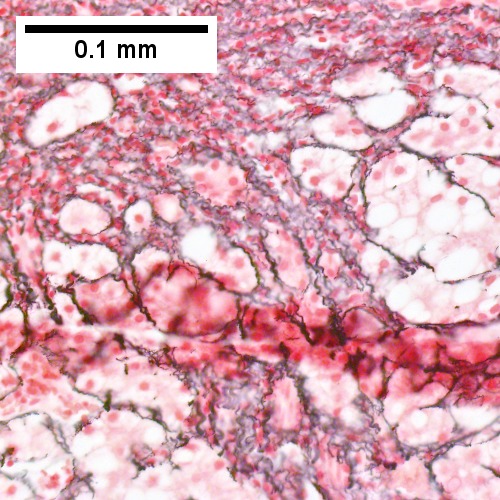
Hepatitis C with metavir stage IV fibrosis (advanced fibrosis/cirrhosis) and confluent piecemeal necrosis. A. Inflamed bands cross hepatocytes with steatosis. B. Trichrome shows extensive bridges. C. Trichrome also documents early nodule formation. D. Reticulin shows regeneration (two nuclei per cord) in a nodule, but not throughout. E. Hematoxylin and eosin shows piecemeal necrosis as inflammatory cells surrounding hepatocytes. F. Reticulin shows black lines about hepatocytes, indicating confluent piecemeal necrosis.
A. 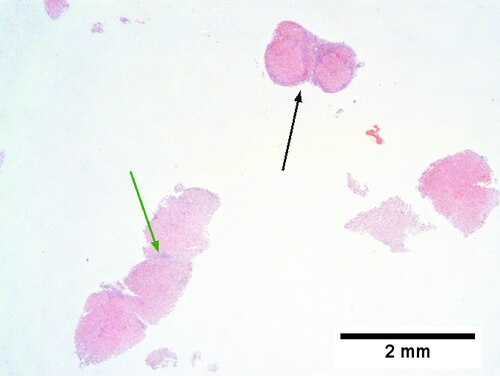
B. 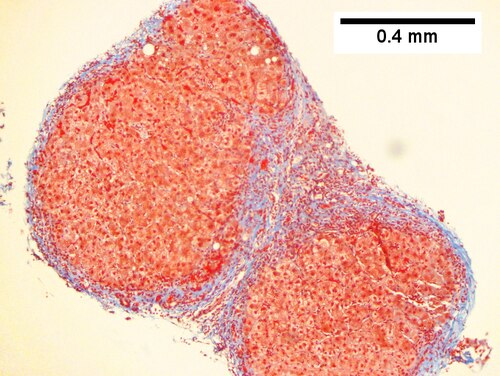
C. 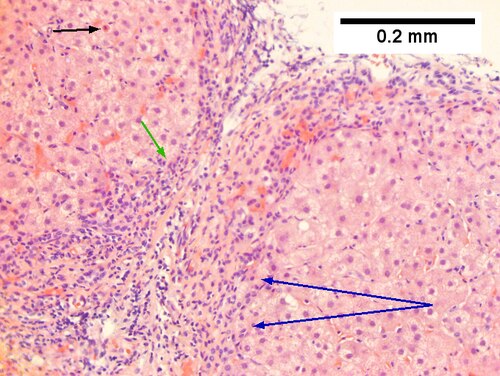
D. 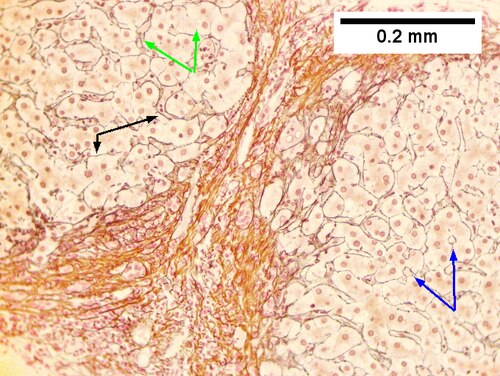
E. Hepatitis C virus. Metavir activity index 3 (PMN 2, LN 2). Metavir stage 4 (cirrhosis, definite by old criteria).
F. Hepatitis C virus. Metavir activity index 3 (PMN 2, LN 2). Metavir stage 4 (cirrhosis, definite by old criteria).
Hepatitis C virus. Metavir activity index 3 (PMN 2, LN 2). Metavir stage 4 (cirrhosis, definite by old criteria). A. Fragmentation raises the suspicion of cirrhosis, especially given absent triads, and an inflamed band [green arrow]; nodules [black arrow] are visible. B. Trichrome stain shows fibrosis about the nodules, whose interface will be examined in remaining images. C. Chronic inflammation shows interface hepatitis [green arrow] as well as surrounding of hepatocytes [blue arrows] for piecemeal necrosis; a necrotic hepatocyte demarcates lobular necrosis [black arrow]. D. Reticulin shows regeneration via two nucleus thick cords [green arrows], but also by rosettes [blue arrows] and, most definite, by overall lack of direction to black lines, going different ways with respect to the edge of the fibrotic, inflamed band [black arrows]; black lines surrounding hepatocytes/hepatocyte groups [black arrows] document continuous piecemeal necrosis. E. PAS without diastase stain on core biopsies can make piecemeal necrosis more obvious than on reticulin by showing stroma bounded red hepatocyte cytoplasm of cells [arrows]. F. PAS with diastase has pink lines to use to evaluate the sinusoidal structure, similar to reticulin, but not as good; note spotty necrosis [black arrow] and proliferated bile ductules [red arrows].
DDx:
- Hepatitis B (without ground glass hepatocytes).
- Autoimmune hepatitis.
- Primary biliary cirrhosis without granulomas.
- Drug reaction.
See also
References
- ↑ STC. 6 December 2010.
- ↑ Yoon EJ, Hu KQ. Hepatitis C virus (HCV) infection and hepatic steatosis. Int J Med Sci. 2006;3(2):53-6. Epub 2006 Apr 1. PMID 16614743. Avialable at: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=1415843. Accessed on: September 9, 2009.
- ↑ OA. September 2009.
- ↑ Johnson, K; Kotiesh, A; Boitnott, JK; Torbenson, M (Nov 2007). "Histology of symptomatic acute hepatitis C infection in immunocompetent adults.". Am J Surg Pathol 31 (11): 5286-96. PMID 18059233.