Papillary renal cell carcinoma
Papillary renal cell carcinoma, abbreviated PRCC, PaRCC and papillary RCC, is the second most common type of renal cell carcinoma.

General
- Often subclassified[1] into type 1 and type 2 -- see microscopic.
- Type 1 and Type 2 are different on a cytogenetic and molecular basis.[2]
Epidemiology
- Associated with acquired renal cystic disease.[3]
- May be familial - uncommon.[4]
- MET mutation[5] - autosomal dominant transmission, PaRCC type 1.
Gross
- Renal cortical mass > 0.5 cm.
- May be multifocal. ‡
- Often necrotic appearing - light-to-dark brown, soft/mushy, friable.
Note:
- ‡ Approximately 10% of PaRCCs are multifocal (based on a set of 5378 patients);[6] it is the renal tumour that is most commonly multifocal.
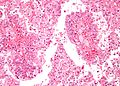
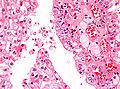
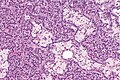
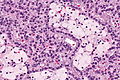
Microscopic
Features:[7]
- Cuboidal or low columnar cell in papillae.
- Interstitial foam cells in vascular cores - key feature.
- Most sensitive and specific feature of PaRCC.[8]
- Highly vascular.
Size criterion:
- Papillary lesions must be >0.5 cm to be called carcinoma; smaller lesions (<=0.5 cm) are called papillary adenomas.[9]
Mnemonic HIP: highly vascular, interstitial foam cells, papillae.
DDx:
- Clear cell RCC.
- Papillary: histiocytes, intracellular hemosiderin, CK7 +ve.
- Clear cell papillary renal cell carcinoma - apical nuclei, usu. no true papillae.
- Metanephric adenoma (esp. solid PaRCC type 1) - no histiocytes, WT-1 +ve.
- Collecting duct carcinoma - esp. PaRCC type 2.
- Urothelial carcinoma.
- Renal papillary adenoma - doesn't fulfill size criterion for PaRCC.
- Acquired cystic disease-associated renal cell carcinoma.
- Renal mucinous tubular and spindle cell carcinoma.
- Hereditary leiomyomatosis and renal cell carcinoma - for type 2 PaRCC; CK7 -ve, prominent eosinophilic nucleoli.
Images

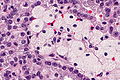
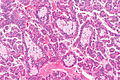
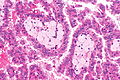
PaRCC - intermed. mag. (WC/Nephron)
PaRCC - high mag. (WC/Nephron)
PaRCC - very high mag. (WC/Nephron)



PaRCC - intermed. mag. (WC)
PaRCC - high mag. (WC)
PaRCC - very high mag. (WC)



PaRCC - high mag. (WC/Nephron)
PaRCC - very high mag. (WC/Nephron)

Histological subtyping
Generally accepted subtypes:[1][10]
- Type 1 - single layer of cells on basement membrane - most important.
- Usually low grade nuclear features, i.e. low ISUP nucleolar grade.
- Other characteristics:
- Clear cytoplasm.
- Foamy macrophages - common.
- Cells smaller.
- Type 2 - pseudostratification of cells - most important.
- Usually high grade nuclear features, i.e. high ISUP nucleolar grade.
- Other characteristics:
- Eosinophilic cytoplasm.
- Foamy macrophages - uncommon.
- Cells larger.
Another subtype:
- Oncocytic - oncocytic cytoplasm.
- Extremely rare ~ largest series is 12 cases.[11]
IHC
Features:[1]
- AMACR +ve.
- HMWCK (34betaE12) +ve.
- Panker (AE1/AE3) +ve.
- CK7 +ve ~90% of type 1, 20% of type 2.
- CD10 +ve.[12]
More reading:
Type 1 versus Type 2:[13]
- CK7:
- Type 1 ~ 100%.
- Type 2 ~ 19%.
- CK19:
- Type 1 ~ 100%.
- Type 2 ~ 53%.
Metanephric adenoma vs. PaRCC type 1:[14]
- AMACR +ve.
- WT-1 -ve.
- CD57 -ve.
Molecular
Features:[15]
- Sporadic: trisomies 7, 16, 17.
- Familial: trisomy 7.
- Chromosome 7 = location of MET gene.
Note:
- Not used for diagnosis.[16]
Sign out
- The 2004 WHO GU (blue) book notes that some pathologists report lesions that are 0.5-2.0 cm as papillary epithelial neoplasm of low malignant potential.[17] Papillary epithelial neoplasm of low malignant potential should not be confused the similarly sounding papillary urothelial lesion (papillary urothelial neoplasm of low malignant potential).
Kidney Tumour, Left, Partial Nephrectomy: - PAPILLARY RENAL CELL CARCINOMA. -- Surgical margins NEGATIVE. -- ISUP nucleolar (Fuhrman) Grade 3. -- TNM stage: pT1a pNx. -- Please see tumour summary.
Block letters
KIDNEY, RIGHT, RADICAL NEPHRECTOMY: - PAPILLARY RENAL CELL CARCINOMA, TYPE 1, ISUP NUCLEOLAR GRADE 3, pT2a(2), pNx. -- SURGICAL MARGINS NEGATIVE. -- PLEASE SEE TUMOUR SUMMARY. - RENAL PAPILLARY ADENOMAS.
Micro
The sections show a tumour in the kidney with fibrovascular cores (papillae) that focally contain macrophages. Psammoma bodies are present. Siderophages are present.
The papillae predominantly have a single layer of tumour cells and the cytoplasm of the tumour cells is predominantly clear.
Nucleoli are visible focally with the 10x objective (ISUP nucleolar grade 3).
A second tumour with the same morphology is present and measures 8 millimetres.
Multiple small lesions, like the largest tumour, less than 0.5 cm are present.
Oncocytic variant
KIDNEY, RIGHT, NEPHRECTOMY: - PAPILLARY RENAL CELL CARCINOMA, ONCOCYTIC -- SEE COMMENT; - FUHRMANN GRADE 2; - SURGICAL MARGINS NEGATIVE; - PLEASE SEE TUMOUR SUMMARY. COMMENT: The oncocytic variant of papillary renal cell carcinoma (RCC) is uncommon and not widely recognized as a subtype of papillary RCC. The prognostic significance of the oncocytic cytoplasm is uncertain.[1] The histomorphology in this case is compatible with a type 1 papillary RCC. 1. Ann Diagn Pathol. 2006 Jun;10(3):133-9.
See also
References
- ↑ 1.0 1.1 1.2 Zhou, Ming; Magi-Galluzzi, Cristina (2006). Genitourinary Pathology: A Volume in Foundations in Diagnostic Pathology Series (1st ed.). Churchill Livingstone. pp. 289. ISBN 978-0443066771.
- ↑ Klatte, T.; Pantuck, AJ.; Said, JW.; Seligson, DB.; Rao, NP.; LaRochelle, JC.; Shuch, B.; Zisman, A. et al. (Feb 2009). "Cytogenetic and molecular tumor profiling for type 1 and type 2 papillary renal cell carcinoma.". Clin Cancer Res 15 (4): 1162-9. doi:10.1158/1078-0432.CCR-08-1229. PMID 19228721.
- ↑ Fogo, Agnes B.; Kashgarian, Michael (2005). Diagnostic Atlas of Renal Pathology: A Companion to Brenner and Rector's The Kidney 7E (1st ed.). Saunders. pp. 438. ISBN 978-1416028710.
- ↑ Czene, K.; Hemminki, K. (Apr 2003). "Familial papillary renal cell tumors and subsequent cancers: a nationwide epidemiological study from Sweden.". J Urol 169 (4): 1271-5. doi:10.1097/01.ju.0000052373.36963.12. PMID 12629341.
- ↑ Wadt, KA.; Gerdes, AM.; Hansen, TV.; Toft, BG.; Friis-Hansen, L.; Andersen, MK. (Sep 2012). "Novel germline c-MET mutation in a family with hereditary papillary renal carcinoma.". Fam Cancer 11 (3): 535-7. doi:10.1007/s10689-012-9542-6. PMID 22717761.
- ↑ Siracusano, S.; Novara, G.; Antonelli, A.; Artibani, W.; Bertini, R.; Carini, M.; Carmignani, G.; Ciciliato, S. et al. (Dec 2012). "Prognostic role of tumour multifocality in renal cell carcinoma.". BJU Int 110 (11 Pt B): E443-8. doi:10.1111/j.1464-410X.2012.11121.x. PMID 22502873.
- ↑ Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 1017-8. ISBN 0-7216-0187-1.
- ↑ Granter SR, Perez-Atayde AR, Renshaw AA (October 1998). <303::AID-CNCR6>3.0.CO;2-7 "Cytologic analysis of papillary renal cell carcinoma". Cancer 84 (5): 303?8. PMID 9801205. http://dx.doi.org/10.1002/(SICI)1097-0142(19981025)84:5<303::AID-CNCR6>3.0.CO;2-7.
- ↑ Zhou, Ming; Magi-Galluzzi, Cristina (2006). Genitourinary Pathology: A Volume in Foundations in Diagnostic Pathology Series (1st ed.). Churchill Livingstone. pp. 288. ISBN 978-0443066771.
- ↑ Delahunt, B.; Eble, JN. (Jun 1997). "Papillary renal cell carcinoma: a clinicopathologic and immunohistochemical study of 105 tumors.". Mod Pathol 10 (6): 537-44. PMID 9195569.
- ↑ Srigley, JR.; Delahunt, B. (Jun 2009). "Uncommon and recently described renal carcinomas.". Mod Pathol 22 Suppl 2: S2-S23. doi:10.1038/modpathol.2009.70. PMID 19494850.
- ↑ http://surgpathcriteria.stanford.edu/kidney/papillary-renal-cell-carcinoma/differential-diagnosis.html. Accessed on: 6 May 2014.
- ↑ Ono, Y.; Ito, T.; Tsujino, S.; Aizawa, S.; Suzuki, M. (Jun 1997). "[A study of papillary renal cell carcinoma. Clinicopathological, immunohistochemical features and its typing].". Nihon Hinyokika Gakkai Zasshi 88 (6): 587-95. PMID 9234615.
- ↑ Watanabe, S.; Naganuma, H.; Shimizu, M.; Ota, S.; Murata, S.; Nihei, N.; Matsushima, J.; Mikami, S. et al. (2013). "Adult nephroblastoma with predominant epithelial component: a differential diagnostic candidate of papillary renal cell carcinoma and metanephric adenoma-report of three cases.". Case Rep Pathol 2013: 675875. doi:10.1155/2013/675875. PMID 24083046.
- ↑ Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 1016. ISBN 0-7216-0187-1.
- ↑ Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 292. ISBN 978-0781765275.
- ↑ The International Agency for Research on Cancer (Author), J. Eble (Editor), J. Epstein (Editor), I. Sesterhenn (Editor), G. Sauter (Editor) (2004). Pathology and Genetics of Tumours of the Urinary System and Male Genital Organs (IARC WHO Classification of Tumours) (1st ed.). Lyon: World Health Organization. pp. 28. ISBN 978-9283224150.