Endometriosis
Endometriosis causes significant morbidity and is associated with increased risk of certain malignancies.
| Endometriosis | |
|---|---|
| Diagnosis in short | |
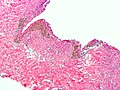
 Endometriosis of the ovary. H&E stain. | |
|
| |
| LM | at least 2 of 3: (1) endometrial glands, (2) endometrial stroma, (3) hemosiderin-laden macrophages |
| LM DDx | adenocarcinoma, endosalpingiosis |
| IHC | CD10 +ve (stroma) |
| Gross | chocolate cyst |
| Site | ovary, uterine ligaments, cul-de-sac, peritoneum, cervix, vagina, fallopian tubes, surgical scars, gastrointestinal tract |
|
| |
| Associated Dx | infertility, endometrioid adenocarcinoma of the ovary, clear cell adenocarcinoma of the ovary, seromucinous borderline tumour |
| Symptoms | pelvic pain |
| Prevalence | common |
| Blood work | CA-125 mildly elevated |
| Prognosis | benign |
General
Pathophysiology
There are several theories for endometriosis, i.e. how it is that endometrial tissue gets found outside of the uterus:
- Retrograde menstruation - probably the most common.[1]
- Ectopic endometrial tissue.[2]
- Coelomic metaplasia.
- Hematogenous spread or lymphatic spread.
Clinical
- A significant cause of infertility.
- A cause of pelvic pain.
- Affects approximately 10% of women of child bearing age.
- Associated with moderate elevation of (serum) CA-125.
Tumours associated with endometriosis
Endometriosis is associated with gynecologic tumours:
- Endometrioid adenocarcinoma of the ovary.[3]
- Clear cell carcinoma of the ovary.[4]
- Endocervical-like mucinous borderline tumour (EMBT).[5]
- Mixture of EMBT and serous borderline tumor = seromucinous borderline tumour.
Other tumours & decreased risk:[6]
- Increased: endocrine tumours, non-Hodgkin's lymphoma, brain tumours.
- Decreased: cervical cancer.
Rare stuff:
- There are case reports of endometriosis in men on estrogen therapy for prostate cancer.[7][8]
Gross
Appearance:
- Chocolate cyst = cyst containing light brown material.
Classic locations:
- Ovary - most common location according to Jenkins et al.[1]
- Utero-sacral ligament.[9]
- Cul-de-sac.[9]
- Broad ligament.
Note:
- The hierarchy of the most common sites, i.e. what is most common and what is the second most common etc., depends on the paper one reads, e.g. compare Jenkins et al[1] with Stegmann et al.[9]
- Robbins gives the order as: ovaries, uterine ligaments, rectovaginal septum, cul-de-sac, pelvic periteoneum, gastrointestinal tract, cervix, vagina, fallopian tubes, laparotomy scars.[10]
- Endometriosis can appear almost any where.
- A well-reported uncommon location is the abdominal wall post-caesarian section.[11]
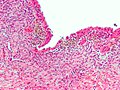
Microscopic
Criteria - need at least 2 / 3 for the diagnosis:[12]
- Endometrial glands - endometrial glands are classically: circular, with nuclei that are hyperchromatic & cigar-shaped.
- Endometrial stroma - endometrial stroma is classically: cellular and hyperchromatic (may resemble a lymphocytic infiltration on low power).
- Hemosiderin-laden macrophages - light brown, may be granular.
Notes:
- The epithelial component (1) may appear cuboidal in cysts or be sloughed-off, i.e. absent.
- The microscopic correlation of chocolate cyst is: light brown acellular material; this can be considered as a substitute for (3) - hemosiderin-laden macrophages.
- Epithelial component may have tubal metaplasia.[13]
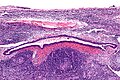
- Endometriosis may mimic cancer[14] - see images below.
- If it is just endometrial type glands - the stroma is missing... it is probably endosalpingiosis.
DDx:
- Adenocarcinoma.
- Endosalpingiosis - does not have stromal component.
- In the GI tract, it classically expands the muscularis propria.
Images

Endometriosis - ovary. (WC/Nephron)
Endometriosis - low mag. (WC/Nephron)
Endometriosis - high mag. (WC/Nephron)


Mimicking cancer:

Endometriosis in the small intestine - low mag. (WC/Nephron)
Endometriosis in a lymph node - intermed. mag. (WC/Nephron)


www:
Immunohistochemical stains
- CD10 +ve -- stains the stromal cells.[15]
- ER +ve -- stains the epithelium.
- CK7 +ve -- stains the epithelium.
- CK20 -ve -- used to exclude colorectal adenocarcinoma.
Sign out
Biopsy
OVARIAN FOSSA, RIGHT, BIOPSY: - ENDOMETRIOSIS. - FIBROADIPOSE TISSUE PARTIALLY COVERED BY MESOTHELIUM.
CYST WALL, OVARY LEFT, CYSTECTOMY: - ENDOMETRIOSIS.
CUL-DE-SAC, BIOPSY: - ENDOMETRIOSIS. COMMENT: A CD10 immunostain marks the endometrial-type stroma and confirms the presence of endometriosis.
Ovary and tube
OVARY AND FALLOPIAN TUBE, LEFT, SALPINO-OOPHORECTOMY: - OVARY WITH ENDOMETRIOSIS. - FALLOPIAN TUBE WITHIN NORMAL LIMITS. - NEGATIVE FOR MALIGNANCY.
TAH-USO
UTERUS, UTERINE TUBES, LEFT OVARY, TOTAL HYSTERECTOMY, BILATERAL SALPINGECTOMY AND LEFT OOPHRECTOMY: - LEIOMYOMATA WITH HYALINE CHANGE. - NONPROLIFERATIVE ENDOMETRIAL GLANDS WITH STROMAL DECIDUALIZATION, AND GLANDULAR DILATION. - LEFT OVARY WITH ENDOMETRIOSIS, SEE COMMENT. - LEFT UTERINE TUBE WITH ENDOMETRIOSIS, SEE COMMENT. - RIGHT UTERINE TUBE WITHIN NORMAL LIMITS. - UTERINE CERVIX WITHIN NORMAL LIMITS. - NEGATIVE FOR MALIGNANCY. COMMENT: The presence of endometrial stroma was demonstrated with CD10 immunostaining, thus confirming the presence of endometriosis.
TAH-BSO
UTERINE CERVIX, UTERUS, UTERINE TUBES AND OVARIES, TOTAL HYSTERECTOMY AND BILATERAL SALPINGOOPHERECTOMY: - UTERINE CERVIX WITHIN NORMAL LIMITS. - PROLIFERATIVE PHASE ENDOMETRIUM. - UTERUS WITH FIBROUS SEROSAL ADHESIONS. - LEFT UTERINE TUBE WITH ENDOMETRIOSIS. - RIGHT UTERINE TUBE WITHIN NORMAL LIMITS. - RIGHT AND LEFT OVARIES WITH ENDOMETRIOSIS.
Micro
The sections show soft tissue with endometrial-type glands surrounded by endometrial-type stroma. Siderophages are present. No nuclear atypia is identified. Mitotic activity is not apparent.
See also
References
- ↑ 1.0 1.1 1.2 Jenkins, S.; Olive, DL.; Haney, AF. (Mar 1986). "Endometriosis: pathogenetic implications of the anatomic distribution.". Obstet Gynecol 67 (3): 335-8. PMID 3945444.
- ↑ Signorile, PG.; Baldi, F.; Bussani, R.; D'Armiento, M.; De Falco, M.; Baldi, A. (2009). "Ectopic endometrium in human foetuses is a common event and sustains the theory of müllerianosis in the pathogenesis of endometriosis, a disease that predisposes to cancer.". J Exp Clin Cancer Res 28: 49. doi:10.1186/1756-9966-28-49. PMID 19358700.
- ↑ Nagle CM, Olsen CM, Webb PM, Jordan SJ, Whiteman DC, Green AC (November 2008). "Endometrioid and clear cell ovarian cancers: a comparative analysis of risk factors". Eur. J. Cancer 44 (16): 2477-84. doi:10.1016/j.ejca.2008.07.009. PMID 18707869.
- ↑ Kawaguchi R, Tsuji Y, Haruta S, et al. (October 2008). "Clinicopathologic features of ovarian cancer in patients with ovarian endometrioma". J. Obstet. Gynaecol. Res. 34 (5): 872–7. doi:10.1111/j.1447-0756.2008.00849.x. PMID 18834345.
- ↑ Moriya T, Mikami Y, Sakamoto K, et al. (December 2003). "Endocervical-like mucinous borderline tumors of the ovary: clinicopathological features and electron microscopic findings". Med Electron Microsc 36 (4): 240–6. doi:10.1007/s00795-003-0221-4. PMID 16228656.
- ↑ URL: http://www.medicalnewstoday.com/articles/3890.php. Accessed on: 26 September 2011.
- ↑ Fukunaga, M. (Jan 2012). "Paratesticular endometriosis in a man with a prolonged hormonal therapy for prostatic carcinoma.". Pathol Res Pract 208 (1): 59-61. doi:10.1016/j.prp.2011.10.007. PMID 22104297.
- ↑ Beckman, EN.; Pintado, SO.; Leonard, GL.; Sternberg, WH. (May 1985). "Endometriosis of the prostate.". Am J Surg Pathol 9 (5): 374-9. PMID 2418693.
- ↑ 9.0 9.1 9.2 Stegmann, BJ.; Sinaii, N.; Liu, S.; Segars, J.; Merino, M.; Nieman, LK.; Stratton, P. (Jun 2008). "Using location, color, size, and depth to characterize and identify endometriosis lesions in a cohort of 133 women.". Fertil Steril 89 (6): 1632-6. doi:10.1016/j.fertnstert.2007.05.042. PMID 17662280.
- ↑ Mitchell, Richard; Kumar, Vinay; Fausto, Nelson; Abbas, Abul K.; Aster, Jon (2011). Pocket Companion to Robbins & Cotran Pathologic Basis of Disease (8th ed.). Elsevier Saunders. pp. 524. ISBN 978-1416054542.
- ↑ Ozel, L.; Sagiroglu, J.; Unal, A.; Unal, E.; Gunes, P.; Baskent, E.; Aka, N.; Titiz, MI. et al. (Mar 2012). "Abdominal wall endometriosis in the cesarean section surgical scar: a potential diagnostic pitfall.". J Obstet Gynaecol Res 38 (3): 526-30. doi:10.1111/j.1447-0756.2011.01739.x. PMID 22381104.
- ↑ Tadrous, Paul.J. Diagnostic Criteria Handbook in Histopathology: A Surgical Pathology Vade Mecum (1st ed.). Wiley. pp. 239. ISBN 978-0470519035.
- ↑ Clement PB (July 2007). "The pathology of endometriosis: a survey of the many faces of a common disease emphasizing diagnostic pitfalls and unusual and newly appreciated aspects". Adv Anat Pathol 14 (4): 241–60. doi:10.1097/PAP.0b013e3180ca7d7b. PMID 17592255.
- ↑ Corben, AD.; Nehhozina, T.; Garg, K.; Vallejo, CE.; Brogi, E. (Aug 2010). "Endosalpingiosis in axillary lymph nodes: a possible pitfall in the staging of patients with breast carcinoma.". Am J Surg Pathol 34 (8): 1211-6. doi:10.1097/PAS.0b013e3181e5e03e. PMID 20631604.
- ↑ Tadrous, Paul.J. Diagnostic Criteria Handbook in Histopathology: A Surgical Pathology Vade Mecum (1st ed.). Wiley. pp. 236. ISBN 978-0470519035.