Actinic keratosis
| Actinic keratosis | |
|---|---|
| Diagnosis in short | |
 | |
|
| |
| LM | basal epidermal atypia - key feature, palisading of basal cells, solar elastosis +/-parakeratosis |
| Subtypes | bowenoid actinic keratosis, hypertrophic actinic keratosis, acantholytic actinic keratosis, proliferative actinic keratosis, pigmented actinic keratosis, lichenoid actinic keratosis |
| LM DDx | squamous cell carcinoma of the skin, Bowen's disease |
| IHC | CK34betaE12 +ve |
| Site | skin |
|
| |
| Associated Dx | squamous cell carcinoma of the skin, Bowen's disease |
| Signs | sandpaper-like texture |
| Prognosis | good |
| Clin. DDx | squamous cell carcinoma, melanoma (for pigmented AK) |
Actinic keratosis, abbreviated AK, is a common skin lesion. It is also known as solar keratosis.[1][2]
General
- Considered a precursor of squamous cell carcinoma of the skin.[2]
Risk factors:[3]
- Sun exposure.
- Immune suppression (e.g. organ transplant recipients).
Gross
Features:
- Yellow-brown scaly, patches.
- Sandpaper sensation - on touching.
- Usually small (<1cm), but larger lesions may occur.
- May be pigmented.[4]
Microscopic
Features:[5]
- Epidermal nuclear atypia:
- Variation is size, shape and staining - must involve basilar layer.
- Nuclear enlargement - key feature.
- Hyperchromasia.
- Variation is size, shape and staining - must involve basilar layer.
- Abnormal epidermal architecture:
- Palisading.[citation needed]
- +/-Parakeratosis - may alternate with orthokeratosis, esp. early lesions.[6]
- +/-Irregular acanthosis.
Note:
- May be full thickness - known as bowenoid actinic keratosis.[7]
DDx:
- Actinic cheilitis - the same lesion on the lip.[8]
- Bowen's disease - full thickness involvement - with involvement of adnexal epithelium and follicular epithelium.[7]
- Paget disease of the breast.
- Squamous cell carcinoma of the skin.
- Lentigo maligna (melanoma in situ on sun damaged skin) - esp. for pigmented AK.[6]
- One should see benign melanocytes within an AK... otherwise one should do stains as the melanocytes may be mimicking keratinocytes.
- Seborrheic keratosis - should not have basilar nuclear atypia.
- Lichenoid keratosis (esp. for lichenoid actinic keratosis) - has a band of inflammatory cells in the superficial dermis.
- Discoid Luphus Erythematosus.
Images
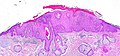
Actinic keratosis. (WC)

Actinic keratosis. (WC)

Actinic keartosis. (WC)
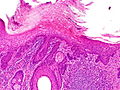
Actinic keratosis. (WC)




Bowenoid actinic keratosis - high mag. (WC)

Bowenoid actinic keratosis - very high mag. (WC)


Histologic subtypes of actinic keratosis
Like most common things, there are several variants:[6]
- Hypertrophic actinic keratosis.
- Increased thickness of: (1) epidermis and, (2) stratum corneum.[9]
- Acantholytic actinic keratosis.
- Proliferative actinic keratosis - downward finger-like projections of the epidermis.
- Pigmented actinic keratosis.
- DDx: lentigo maligna.
- Lichenoid actinic keratosis - band of inflammatory cells at the dermal-epidermal junction.
- DDx: lichen planus.
- Atrophic actinic keratosis.
Sign out
Left Ear Skin Lesion, Biopsy: - Hypertrophic squamous lesion, possibly hypertrophic actinic keratosis, see comment. - Solar elastosis, marked. Comment: The lesion has mild basal atypia, proliferative activity and marked hyperkeratosis. The lesion extends to the edge of the tissue and may not be representative of the lesion seen clinically. Clinical correlation is required. Re-excision to rule-out un-sampled pathology should be considered.
All uppercase
SKIN LESION, RIGHT THIGH, BIOPSY: - HYPERTROPHIC ACTINIC KERATOSIS. - SOLAR ELASTOSIS. - NEGATIVE FOR MALIGNANCY.
Bowenoid
SKIN LESION, RIGHT DISTAL FOREARM, BIOPSY: - BOWENOID ACTINIC KERATOSIS, COMPLETELY EXCISED IN PLANE OF SECTION. - EXTENSIVE SOLAR ELASTOSIS. - NEGATIVE FOR MALIGNANCY.
Micro
General
The sections show skin with basilar epidermal nuclear enlargement and hyperchromasia with irregular nuclear palisading. Hyperkeratosis and parakeratosis is present. A granular layer is present. The dermal-epidermal interface is sharply-demarcated. There is focal inflammation at the interface. Extensive solar elastosis is present.
There is no clefting of the lesion from the surrounding stroma. The surrounding stroma does not have a myxoid quality.
Bowenoid
The sections show skin with epidermal nuclear enlargement and hyperchromasia with irregular nuclear palisading. The lesion involves the full thickness of the epidermis; however, it spares adnexal and follicular epithelium. Proliferative activity is present. Hyperkeratosis and parakeratosis is present. A granular layer is present. The dermal-epidermal interface is sharply-demarcated. There is focal inflammation at the interface. Extensive solar elastosis is present.
There is no clefting of the lesion from the surrounding stroma. Intercellular bridges are identified.
Lichenoid AK
The sections show skin with a lymphoplasmacytic interface dermatitis, hypergranulosis, hyperkeratosis, loss of the rete ridges and apoptotic keratinocytes. The epidermis matures to the surface; however, there is basal cell hyperplasia associated with moderate keratinocyte nuclear atypia (including hyperchromasia and anisonucleosis). Pigment incontinence is present. Solar elastosis is present. The lesion is completely excised in the plane of section.
See also
References
- ↑ Weinberg, JM. (Jan 2006). "Topical therapy for actinic keratoses: current and evolving therapies.". Rev Recent Clin Trials 1 (1): 53-60. PMID 18393780.
- ↑ 2.0 2.1 Roewert-Huber, J.; Stockfleth, E.; Kerl, H. (Dec 2007). "Pathology and pathobiology of actinic (solar) keratosis - an update.". Br J Dermatol 157 Suppl 2: 18-20. doi:10.1111/j.1365-2133.2007.08267.x. PMID 18067626.
- ↑ Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 1180. ISBN 978-1416031215.
- ↑ URL: http://www.dermoscopy-ids.org/index.php/newest-case/79-lentigo-maligna-vs-pigmented-actinic-keratosis. Accessed on: 23 August 2012.
- ↑ URL: http://emedicine.medscape.com/article/1099775-workup#a0723. Accessed on: 1 September 2011.
- ↑ 6.0 6.1 6.2 Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 353. ISBN 978-0443066542.
- ↑ 7.0 7.1 Bagazgoitia, L.; Cuevas, J.; Juarranz, A. (Feb 2010). "Expression of p53 and p16 in actinic keratosis, bowenoid actinic keratosis and Bowen's disease.". J Eur Acad Dermatol Venereol 24 (2): 228-30. doi:10.1111/j.1468-3083.2009.03337.x. PMID 19515076.
- ↑ Picascia, DD.; Robinson, JK. (Aug 1987). "Actinic cheilitis: a review of the etiology, differential diagnosis, and treatment.". J Am Acad Dermatol 17 (2 Pt 1): 255-64. PMID 3305604.
- ↑ Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 352. ISBN 978-0443066542.