Microorganisms
Microorganisms show-up every once in a while. It is essential to know 'em.
Microorganisms
| Name (disease) | Kingdom | Size | Shape | Stains | Other (microscopic) | Clinical | References | Image |
|---|---|---|---|---|---|---|---|---|
| Aspergillus (aspergillosis) | Fungi | ? | Hyphae that branching with 45 degrees angle |
PAS-D | Fruiting heads when aerobic | ? Immunosuppression | [1] | Aspergillus (WC), Aspergillus cytology (WC) |
| Zygomycota (zygomycosis); more specific Mucorales (mucormycosis) |
Fungi | ? | Branching hyphae with variable width | ? | Granulomata assoc. | Diabetes, immunodeficient | [1] | Mucormycosis (homestead.com), Zygomycosis (WC) |
| Coccidioides, usually C. immitis (coccidioidomycosis) |
Fungi | Large - 20-60 micrometers, endospores 1-5 micrometers |
Spherules | Stains? | Other? | Immunodeficient | [1] | Coccidioidomycosis (med.sc.edu) C. immitis (WC) |
| Histoplasma (histoplasmosis) | Fungi | 2-5 micrometers | Spherical | GMS | Intracellular (unlike candida), granulomata | Source: soil with bird droppings | [1] | Histoplasmosis (WC) |
| Blastomyces (Blastomycosis) | Fungi | 5-15 micrometres | Spherical (yeast) | Stains? | Granulomas, broad-based budding yeast | Habitat: Northeast America, Africa | [1][2] | Blastomyces |
| Paracoccidioides (Paracoccidioidomycosis) | Fungi | 6-60 micrometres | Spherical (yeast) | Stains? | Multiple budding "steering wheel" appearance | Clinical??? | [1] | P. brasiliensis (WC). |
| Pneumocystis jirovecii (Pneumocystis carinii pneumonia; abbrev. PCP) | Fungi (previously thought to be a protozoan) | 7-8 micrometres | "Dented ping-pong ball" | GMS | Usually in clusters of alveolar casts with a honeycomb appearance | HIV/AIDS associated | [3] | PCP (WC) |
| Cryptococcosis | Fungi | 5-15 micrometres | Yeast | GMS | Prominent (i.e. thick polysaccharide) capsule | HIV/AIDS associated, most common CNS fungus | [1] | Crytococcosis - methenamine silver (WC), Crytococcosis - mucicarmine (WC). |
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Notes:
- Bold text = key features.
Fungi
- There are lots of 'em. Below are a few of 'em.
Terminology:[4]
- Hyphae = microscopic filamentous growth (of fungi) -- single cell.
- Mycelial = filamentous network of hyphae.
- Septae/septation = hyphae may be subdivided by septae -- if they aren't they are one mass of protoplasm. (?)
- Dimorphism = exist in two forms; e.g. single cell (yeast) and mycelial growth.
- Pseudohyphae = looks like hyphae --but branching pattern is created by separate cells.[5]
Tissue invasive fungi
Typically:[6]
- Mucor
- Aspergillus
Histoplasmosis
- Histoplasma capulatum - primative fungus, typical location: lung.
- Often in yeast form in tissue 2-5 micrometres.[7]
- Nice bright red on PAS-D - histoplasmosis (wikipedia.org).
- Have a "central dot"[8] - histoplasma (ouhsc.edu).
{kind=link}
{kind=link}
Coccidiomycosis
- Coccidioides immitis - fungus, from soil, typical locations: lung, oral cavity.[9]
- Forms spherules 60-80 micrometres in size.[7]
- Coccidioides (commons.wikimedia.org).
{kind=link}
Pneumocystis pneumonia (PCP)
- Pneumocystis jirovecii (used to be called Pneumocystis carinii) - fungus (that used to be considered a parasite), typical location: lung.
- Clinical: Opportunistic infection. May have subtle finding on chest x-ray.
- "Dented ping-pong ball" appearance;[7] - remember PCP = ping-pong.
- Approximately 7-8 micrometres in size - PCP (WP). Several images are here (WC).
Cryptococcus
- Usually C. neoformans, fungus - opportunistic infection, typical location: lung.
- Most common fungus seen in CSF specimens.[1]
Appearance:
- Yeast:
Images:
- Micrograph of crytococcosis - mucicarmine stain (WC).
- Micrograph of crytococcosis - methenamine silver stain (WC).
Notes:
- May be confused with corpora amylacea in the CNS, esp. as they (like cryptococci) stain for methenamine silver, Alcian blue, and PAS.[10]
Cryptosporidiosis
General
- Caused by cryptosporidium.
- Fecal-oral transmission.
- Usu. in immunoincompetent individuals, e.g. HIV/AIDS.
Microscopic
Features:
- Uniform spherical nodules 2-4 micrometres in diameter, typical location - GI tract brush border.
- Bluish staining of brush border key feature - low power.
Images:
- Micrograph of cryptosporidium in the gallbladder (hennepin.mn.us).
- Schematic picture of cryptosporidium & bowel (tulane.edu).
- Micrograph of cryptosporidiosis (brown.edu).
- Cryptosporidium - colon (sciencephoto.com).
{kind=link}
Notes:
- Cryptosporidium parvum?[11]
Candidiasis
- Commonly Candida albicans - yeast (fungus), locations: oral cavity, vagina.
- Dimorphic - seen in two forms:
- Stains: PAS, methenamine silver.
- Images:
{kind=link}
{kind=link}
Blastomycosis
- Usually Blastomyces dermatitidis - fungus.
- May be in the oral cavity.[9]
- Histology = Broad-based budding yeast -- is Blastomyces.[13]
- The interface between two separating fungi, i.e. fungi in the process of reproducing, is very large.
- Images:
{kind=link}
{kind=link}
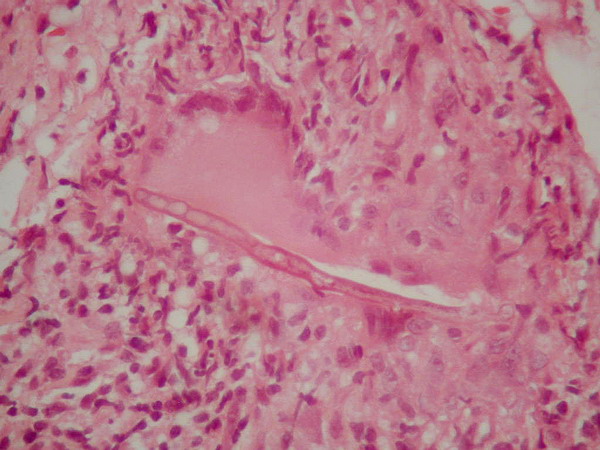
Mucormycosis
General
- Causative organism: Mucorales.
- Kingdom: Fungi.
- AKA Zygomycota (zygomycosis).
- Assoc. with diabetes, immunodeficiency.
Histology
Features:[1]
- Branching hyphae variable width.
- Granulomata associated.
Image:
Worms & stuff
Schistosoma
- See Urine cytopathology.
- Associated with squamous cell carcinoma of the bladder.
Microscopic
Features of ova:
- Elliptical ~80 micrometres max dimension.
- S. haematobium has a "spike" approx. the size of a PMN.
Image:
{kind=link}
Toxoplasma
General
- Common CNS infection.
- Toxoplasma gondii - pathogenic; causes toxoplasmosis.
- Protozoa.
Microscopic
General:
- Dependent on location in body.
Lymph node
LN features:[14]
- Reactive germinal centers (pale areas - larger than usual).
- Often poorly demarcated - due to loose epithelioid cell clusters at germinal center edge - key feature.
- Epithelioid cells - perifollicular & intrafollicular.
- Loose aggregates of histiocytes (do not form round granulomas):
- Abundant pale cytoplasm.
- Nucleoli.
- Loose aggregates of histiocytes (do not form round granulomas):
- Monocytoid cells (monocyte-like cells) - in cortex & paracortex.
- Large cells in islands/sheets key feature with:
- Abundant pale cytoplasm - important.
- Well-defined cell border - important.
- Singular nucleus.
- Cell clusters usually have interspersed neutrophils.
- Large cells in islands/sheets key feature with:
Images (lymph node):
{kind=link}
{kind=link}
CNS
CNS features:[15]
- Granular appearing ball ~ 2x the size of resting lymphocyte.
Images (CNS):
- CNS toxoplasmosis - very high mag. (WC).
- CNS toxoplasmosis - IHC - very high mag. (WC).
- CNS toxoplasmosis (ouhsc.edu).
- CNS toxoplasmosis (ouhsc.edu).
{kind=link}
{kind=link}
IHC
- IHC for toxoplasma.[16]
Strongyloidiasis
General
- Causes by worm Strongyloides stercoralis.
- High case mortality rate ~ 70%.[17]
- May present after years of latency due to immune suppression.[18]
Location:
- Lung. (???)
Microscopic
Features:
- Long worms.
- ~10-15 micrometers wide.
Images:
{kind=link}
Echinococcus
- Several species - most common: Echinococcus granulosus.
- Causes hydatid disease in the liver.
Microscopic
Features:
Enterobius vermicularis
- AKA pinworm.
Features:[21]
- Ovoid eggs - double walled shells, one side flat.
Images:
{kind=link}
Trichinella
General
- Causes Trichinosis.
- Classically associated with uncooked pork.[22]
- Several types; most due to T. spiralis.[22]
Microscopic
Features:
- Worm.
Image:
{kind=link}
Cysticercosis
General
Viruses
Main article: Viruses
This is a fairly big topic. There are about half a dozen viral inclusions (e.g. CMV, HSV, VZV, adenovirus) a decent pathologist ought to be able to identify. The virus article covers 'em.
See also
References
- ↑ 1.00 1.01 1.02 1.03 1.04 1.05 1.06 1.07 1.08 1.09 1.10 Lefkowitch, Jay H. (2006). Anatomic Pathology Board Review (1st ed.). Saunders. pp. 682. ISBN 978-1416025887.
- ↑ http://pathmicro.med.sc.edu/mycology/mycology-6.htm
- ↑ Lefkowitch, Jay H. (2006). Anatomic Pathology Board Review (1st ed.). Saunders. pp. 684. ISBN 978-1416025887.
- ↑ http://www.fungionline.org.uk/1intro/3growth_forms.html
- ↑ http://pathmicro.med.sc.edu/mycology/mycology-3.htm
- ↑ CM 17 Apr 2009.
- ↑ 7.0 7.1 7.2 Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 103. ISBN 978-0781765275.
- ↑ URL: http://moon.ouhsc.edu/kfung/jty1/opaq/PathQuiz/A6I001-PQ01-M.htm. Accessed on: 19 October 2010
- ↑ 9.0 9.1 9.2 Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 3. ISBN 978-0781765275.
- ↑ URL: http://flylib.com/books/en/2.953.1.17/1/. Accessed on: 15 December 2010.
- ↑ http://www.dpd.cdc.gov/dpdx/HTML/Cryptosporidiosis.htm
- ↑ http://pathmicro.med.sc.edu/mycology/mycology-3.htm
- ↑ PMID 12375640
- ↑ Ioachim, Harry L; Medeiros, L. Jeffrey (2008). Ioachim's Lymph Node Pathology (4th ed.). Lippincott Williams & Wilkins. pp. 113. ISBN 978-0781775960.
- ↑ URL: http://moon.ouhsc.edu/kfung/jty1/opaq/PathQuiz/N0I001-PQ01-M.htm. Accessed on: 19 October 2010.
- ↑ URL: http://moon.ouhsc.edu/kfung/jty1/opaq/PathQuiz/N0I001-PQ01-M.htm. Accessed on: 19 October 2010.
- ↑ Lim, S.; Katz, K.; Krajden, S.; Fuksa, M.; Keystone, JS.; Kain, KC. (Aug 2004). "Complicated and fatal Strongyloides infection in Canadians: risk factors, diagnosis and management.". CMAJ 171 (5): 479-84. doi:10.1503/cmaj.1031698. PMID 15337730.
- ↑ Siddiqui, AA.; Berk, SL. (Oct 2001). "Diagnosis of Strongyloides stercoralis infection.". Clin Infect Dis 33 (7): 1040-7. doi:10.1086/322707. PMID 11528578.
- ↑ Mitchell, Richard; Kumar, Vinay; Fausto, Nelson; Abbas, Abul K.; Aster, Jon (2011). Pocket Companion to Robbins & Cotran Pathologic Basis of Disease (8th ed.). Elsevier Saunders. pp. 448. ISBN 978-1416054542.
- ↑ http://www.thefreedictionary.com/scoleces. Accessed on: 10 January 2010.
- ↑ Lefkowitch, Jay H. (2006). Anatomic Pathology Board Review (1st ed.). Saunders. pp. 685. ISBN 978-1416025887.
- ↑ 22.0 22.1 Kaewpitoon N, Kaewpitoon SJ, Philasri C, et al. (October 2006). "Trichinosis: epidemiology in Thailand". World J. Gastroenterol. 12 (40): 6440–5. PMID 17072975. http://www.wjgnet.com/1007-9327/12/6440.asp.
- ↑ URL: http://library.med.utah.edu/WebPath/EXAM/IMGQUIZ/msfrm.html. Accessed on: 5 December 2010.
- ↑ Prasad KN, Prasad A, Verma A, Singh AK (November 2008). "Human cysticercosis and Indian scenario: a review". J. Biosci. 33 (4): 571–82. PMID 19208982.