C-cell hyperplasia
Jump to navigation
Jump to search
| C-cell hyperplasia | |
|---|---|
| Diagnosis in short | |
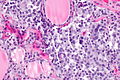
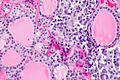
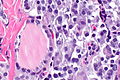
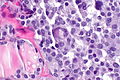
 C-cell hyperplasia. H&E stain. | |
| LM DDx | medullary thyroid carcinoma |
| IHC | CEA +ve, chromogranin A +ve, synaptophysin +ve |
| Gross | not apparent |
| Site | thyroid gland |
|
| |
| Syndromes | Multiple endocrine neoplasia type 2A, Multiple endocrine neoplasia type 2B |
|
| |
| Clinical history | +/-family history of thyroid cancer or MEN 2A or MEN 2B |
| Signs | +/-marfanoid habitus (seen in MEN 2B) |
| Prevalence | uncommon |
| Blood work | calcitonin level elevated |
| Prognosis | benign in itself |
| Treatment | prophylatic surgery |
C-cell hyperplasia, abbreviated CCH, is a pathology of the thyroid gland and considered the precursor for medullary thyroid carcinoma.
General
- Screening for C-cell hyperplasia/medullary thyroid carcinoma done with serum calcitonin level.[1]
Associated with:
- Multiple endocrine neoplasia type 2A[2] - may be found in specimen of a surgery done to exclude MTC in the context of MEN 2A.[3]
- Multiple endocrine neoplasia type 2B.[4]
Gross
- Not visible.
Microscopic
Features:
- Location:[5]
- Mid portion of lobe to upper third of lobe.
- Not at the poles.
- Not in the isthmus.
- Mid portion of lobe to upper third of lobe.
- Definitions vary.[6]
- One definition - either of the following:[1]
- >50 C-cells per low-power field (x100).
- This part of the definition suffers from LPFitis.
- "Medullary thyroid carcinoma confined to the thyroid gland and no larger than 10 mm in greatest dimension."
- >50 C-cells per low-power field (x100).
- Another definition:
- Invasion of the basement membrane with stromal reaction.
- A third definition:
- "Several clusters" of more than six C cells.
- One definition - either of the following:[1]
Images
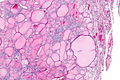
CCH in MEN - very low mag. (WC)
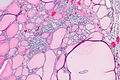
CCH in MEN - low mag. (WC)
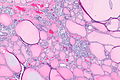
CCH in MEN - low mag. (WC)
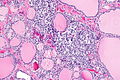
CCH in MEN - intermed. mag. (WC)
CCH in MEN - high mag. (WC)
CCH in MEN - high mag. (WC)
CCH in MEN - very high mag. (WC)
CCH in MEN - very high mag. (WC)








CCH in MEN - chromo A - intermed. mag. (WC)
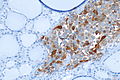
CCH in MEN - chromo A - high mag. (WC)

CCH in MEN - chromo A - very high mag. (WC)

CCH in MEN - CEA - low mag. (WC)
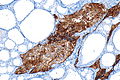
CCH in MEN - CEA - intermed. mag. (WC)

CCH in MEN - CEA - high mag. (WC)

CCH in MEN - CEA - very high mag. (WC)







www
- CCH - crappy B&W image (nature.com).[7]
- CCH - crappy B&W image (nature.com).
- CCH (forpath.org).[8]
- CCH (unibas.ch).
- Nodular CCH (unibas.ch).
{kind=link}
IHC
- Chromogranin A +ve.
- CEA +ve.
- Synaptophysin +ve.
See also
References
- ↑ 1.0 1.1 Machens A, Hoffmann F, Sekulla C, Dralle H (December 2009). "Importance of gender-specific calcitonin thresholds in screening for occult sporadic medullary thyroid cancer". Endocr. Relat. Cancer 16 (4): 1291–8. doi:10.1677/ERC-09-0136. PMID 19726541. http://erc.endocrinology-journals.org/cgi/content/full/16/4/1291.
- ↑ Tyer, NM.; Braunstein, GD.; Frishberg, D.. "Unusual case of multiple endocrine neoplasia type 2A syndrome without medullary thyroid carcinoma.". Endocr Pract 17 (2): e4-7. doi:10.4158/EP10157.CR. PMID 21134882.
- ↑ Etit, D.; Faquin, WC.; Gaz, R.; Randolph, G.; DeLellis, RA.; Pilch, BZ. (Nov 2008). "Histopathologic and clinical features of medullary microcarcinoma and C-cell hyperplasia in prophylactic thyroidectomies for medullary carcinoma: a study of 42 cases.". Arch Pathol Lab Med 132 (11): 1767-73. doi:10.1043/1543-2165-132.11.1767. PMID 18976013.
- ↑ Pagon, RA.; Adam, MP.; Ardinger, HH.; Wallace, SE.; Amemiya, A.; Bean, LJH.; Bird, TD.; Fong, CT. et al. Multiple Endocrine Neoplasia Type 2. PMID 20301434.
- ↑ URL: http://www.cap.org/apps/docs/committees/cancer/cancer_protocols/2011/Thyroid_11protocol.pdf. Accessed on: 7 April 2012.
- ↑ Raphael S. 17 January 2011.
- ↑ Guyétant, S.; Josselin, N.; Savagner, F.; Rohmer, V.; Michalak, S.; Saint-André, JP. (Aug 2003). "C-cell hyperplasia and medullary thyroid carcinoma: clinicopathological and genetic correlations in 66 consecutive patients.". Mod Pathol 16 (8): 756-63. doi:10.1097/01.MP.0000081727.75778.0C. PMID 12920219.
- ↑ URL: http://www.forpath.org/workshops/0201/html/case_7.asp. Accessed on: 21 May 2013.