Muscularis propria invasion in the urinary bladder
The presence or absence of muscularis propria invasion in the urinary bladder is a very important determination, as the clinical management changes between T1 and T2:
- T1: usually conservative treatment (local excision).
- T2: radical treatment (cystectomy or cystoprostatectomy).
A thin layer of discontinous muscularis mucuosae (MM) is present and, especially if hypertrophic, may be confused with muscuaris propria (MP).
General
Comparing muscularis propria and muscularis mucosae
A comparison between muscularis propria and muscularis mucosae - adapted from Paner et al.:[1]
| Feature | Muscularis mucosae | Muscularis propria |
|---|---|---|
| Outline/border | typically irregular (frayed edges) | usually regular (circumscribed) |
| Size of bundles ‡ | classically "small", often "large" (hypertrophic) | usually "large" |
| Isolated fibres | yes | no |
| Location in bladder | less common in trigone, dome very common | everywhere |
| Depth † | superficial, occ. deep | deep |
Notes:
- † The lamina propria thickness varies with location. It is thinnest in the trigone (0.5-1.6 mm) and thickest in the dome (1.0-3.1 mm).
- ‡ Small is defined as <4 muscle fibres; large >= 4 muscle fibres.
- The presence of hyperplastic bundles ranges from ~20% in the trigone to ~70% in the dome.
Images
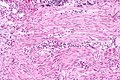
MM - intermed. mag. (wc)
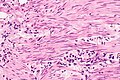
MM - high mag. (WC)
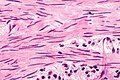
MM - very high mag. (WC)



Microscopic
Rational assessment of muscularis propria invasion
To call muscularis propria invasion:
- Definite tumour must be between muscle.
- Muscle bundles must be thick.
- Multiple bundles must be adjacent to one another.
- Should not be superficial - surface epithelium if present should be distant.
Sign out
Cannot exclude MP invasion
Urinary Bladder Tumour, Transurethral Resection: - INVASIVE HIGH-GRADE UROTHELIAL CARCINOMA. -- Extensive invasion into at least the lamina propria. -- Negative for definite muscularis propria, see comment. Comment: The tumour is seen around bundles of smooth muscle that are favoured to represent muscularis mucosa; however, obliterated muscularis propria cannot be excluded. Correlation with the clinical findings is required. Additional transurethral sampling and/or imaging is suggested.
See also
References
- ↑ Paner, GP.; Ro, JY.; Wojcik, EM.; Venkataraman, G.; Datta, MW.; Amin, MB. (Sep 2007). "Further characterization of the muscle layers and lamina propria of the urinary bladder by systematic histologic mapping: implications for pathologic staging of invasive urothelial carcinoma.". Am J Surg Pathol 31 (9): 1420-9. doi:10.1097/PAS.0b013e3180588283. PMID 17721199.