Difference between revisions of "Odontogenic tumours and cysts"
(→Identifying stuff: +image) |
(→Images: more) |
||
| Line 167: | Line 167: | ||
<gallery> | <gallery> | ||
Image: | Image: Ameloblastoma - low mag.jpg | Ameloblastoma - low mag. (WC) | ||
Image: | Image: Ameloblastoma - intermed mag.jpg | Ameloblastoma - intermed. mag. (WC) | ||
Image: Ameloblastoma - high mag.jpg | Ameloblastoma - high mag. (WC) | |||
Image: Ameloblastoma - very high mag.jpg | Ameloblastoma - very high mag. (WC) | |||
</gallery> | </gallery> | ||
====Morphology==== | ====Morphology==== | ||
*Not prognostic. | *Not prognostic. | ||
Revision as of 20:45, 26 July 2013
This article covers odontogenic tumours and cysts, which is a subset of oral pathology and can be grouped under the heading of head and neck pathology.
The general topic of head and neck pathology is covered in the head and neck pathology and head and neck cytopathology articles.
The vast majority of oral malignancies are squamous cell carcinoma. Common odontogenic cysts are dentigerous cysts, and radicular cysts.[1]
Tooth histology 101
Teeth develop from a combination of:
- Epithelium (downward growth).
- Mesenchyme.
Identifying stuff
Pulp:
- Paucicellular.
- Pale staining.
Enamel:
- Hyperchromatic (dark purple).
- "Fish scale" appearance.
Image:

Tooth. (WC)

Enamel 101
- Arises from reduced enamel epithelium.
Reduced enamel epithelium
Microscopic
Features:
- Bilayered epithelium consisting of:
- Cuboidal/columnar cells with:
- Moderate eosinophilic cytoplasm.
- Round (slightly irregular) centrally place nuclei.
- Cuboidal/columnar cells with:
Notes:
- Transforms into squamous epithelium. (???)
Specific entities
Odontoma
General
- Usually diagnosed clinically.
- Benign.
- Most common odontogenic tumour - considered to be a hamartoma.[2]
- Etiology unknown.[3]
- Typically first two decades of life.
Classification:[2]
- Compound odontoma - tooth-like structure.
- Complex odontoma - disorganized mass of odontogenic tissues.
Microscopic
Features:[2]
- Dentin.
- Cementum.
- Pulpal tissue.
- Enamel - has a "fish-scale" appearance.
- Usually lost during decalcificiation.
Images:
Radicular cyst
- AKA periapical cyst.
Clinical
- Non-vital tooth - key feature.
- The tooth that has lost its nerve.
Microscopic
Features:
- Squamous epithelium - non-keratinized - important.
- +/-Giant cells.
- +/-Cholesterol clefts.
- +/-Abundant plasma cells.
DDx:
- Dentigerous cyst - history is the key to differentiate.
- Keratocystic odontogenic tumour - keratinized epithelium.
- Plasma cell neoplasm[4] - should be considered if the lesion is not associated with a carious tooth.
Dentigerous cyst
General
- Unerupted tooth - usually wisdom teeth.
- Young adults.
Treatment:
- Complete removal - as may transform to squamous cell carcinoma or ameloblastoma.[5]
Gross
- Lesion at crown of tooth.
Microscopic
Features:
- Squamous epithelium.
- Classically described as non-keratinized - in which case the diagnosis is straight forward - important.
- Approximately half have keratin.[6]
- +/-Giant cells.
- +/-Cholesterol clefts.
DDx:
- Radicular cyst - history is the key to differentiate.
- Keratocystic odontogenic tumour - parakeratosis, ribbon like, (artefactual) clefting.
Images:
Sign out
Keratinized
MAXILLARY SINUS CYST, LEFT, EXCISION: - ACANTHOTIC STRATIFIED SQUAMOUS EPITHELIUM WITH INFLAMMATION, COMPACT KERATIN AND FOCAL PARAKERATOSIS -- CONSISTENT WITH DENTIGEROUS CYST WITH KERATIN. - BENIGN BONE. - NEGATIVE FOR ODONTOGENIC KERATOCYSTIC TUMOUR (ODONTOGENIC KERATOCYST).
Keratocystic odontogenic tumour
Ameloblastoma
General
- Osteous lesion.
- Usually mandible.[8]
- In a review of 3677 cases, the mandible-to-maxilla ratio was 5 to 1.[9]
- May arise from an odontogenic cyst,[10] e.g. dentigerous cyst.[7]
Classification
Location:
- Intra-osseous.
- Locally aggressive.
- Peripheral.
- Benign.
Subclassification of intra-osseous type
Histology:
- Solid/multicystic.
- More commonly reoccur.
- Unicystic.
- Unlikely to reoccur.
- Classically found in younger individuals.
Microscopic
Features:[11]
- Stellate reticulum - star-shaped cells, found in a developing tooth.
- Tall columnar cells.
- Palisaded nuclei with reverse polarization.
- Reverse polarization of nuclei = nuclei distant from the basement membrane/nuclei at pole opposite of basement membrane.
- Palisaded nuclei = picket fence appearance; columnar-shaped nuclei with long axis perpendicular to the basement membrane -- key feature.
- Subnuclear vacuolization.
- Palisaded nuclei with reverse polarization.
- +/-Giant cells.
- +/-Subepithelial hyalinization (eosinophilic acellular amorphous material).
- Seen deep to the basement membrane.
- Variable morphology (see below - morphology).
DDx (nuclear palisading):
Images
www:
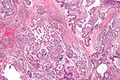
Ameloblastoma - low mag. (WC)
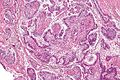
Ameloblastoma - intermed. mag. (WC)
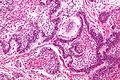
Ameloblastoma - high mag. (WC)
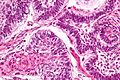
Ameloblastoma - very high mag. (WC)




{kind=link}
Morphology
- Not prognostic.
Morphologic variants:
- Follicular ameloblastoma (classic appearance).
- Plexiform ameloblastoma (does not have prominent palisading).
- Acanthomatous ameloblastoma.
- Desmoplastic ameloblastoma.
- Basaloid ameloblastoma.
Adenomatoid odontogenic tumour
General
- Paedatric population.
Microscopic
Features:
- Palisaded nuclei.
- Whorled epithelium.
Notes:
- No stellate reticulum.
DDx:
Image:
Ameloblastic fibroma
General
- Paedatric population.
Microscopic
Features:
- Palisaded nuclei.
- Fibrous stroma.
Notes:
- No stellate reticulum.
DDx:
Odontogenic myxoma
General
- Benign tumour of mesenchymal origin.
- Often reoccurs.
- Radiologic DDx includes ameloblastoma.
Gross
- Gelatinous mass.
Microscopic
Features:
- Paucicellular lesion with pale staining.
See also
References
- ↑ Eichhorn, W.; Wehrmann, M.; Blessmann, M.; Pohlenz, P.; Blake, F.; Schmelzle, R.; Heiland, M. (Apr 2010). "Metastases in odontogenic cysts: literature review and case presentation.". Oral Surg Oral Med Oral Pathol Oral Radiol Endod 109 (4): 582-6. doi:10.1016/j.tripleo.2009.11.013. PMID 20303056.
- ↑ 2.0 2.1 2.2 2.3 Nelson, BL.; Thompson, LD. (Dec 2010). "Compound odontoma.". Head Neck Pathol 4 (4): 290-1. doi:10.1007/s12105-010-0186-2. PMID 20533004.
- ↑ Yadav, M.; Godge, P.; Meghana, SM.; Kulkarni, SR. (Apr 2012). "Compound odontoma.". Contemp Clin Dent 3 (Suppl 1): S13-5. doi:10.4103/0976-237X.95095. PMID 22629054.
- ↑ Dhanrajani, PJ.; Abdulkarim, SA.. "Multiple myeloma presenting as a periapical lesion in the mandible.". Indian J Dent Res 8 (2): 58-61. PMID 9495138.
- ↑ Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 748. ISBN 978-1416031215.
- ↑ Yoshiura, K.; Higuchi, Y.; Araki, K.; Shinohara, M.; Kawazu, T.; Yuasa, K.; Tabata, O.; Kanda, S. (Jun 1997). "Morphologic analysis of odontogenic cysts with computed tomography.". Oral Surg Oral Med Oral Pathol Oral Radiol Endod 83 (6): 712-8. PMID 9195629.
- ↑ 7.0 7.1 Moosvi, Z.; Tayaar, SA.; Kumar, GS. (Apr 2011). "Neoplastic potential of odontogenic cysts.". Contemp Clin Dent 2 (2): 106-9. doi:10.4103/0976-237X.83073. PMC 3180832. PMID 21957386. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3180832/.
- ↑ URL: http://www.waent.org/archives/2010/Vol3-2/20100618-ameloblastoma/jaw-tumor.htm. Accessed on: 30 November 2011.
- ↑ Reichart, PA.; Philipsen, HP.; Sonner, S. (Mar 1995). "Ameloblastoma: biological profile of 3677 cases.". Eur J Cancer B Oral Oncol 31B (2): 86-99. PMID 7633291.
- ↑ Eversole, LR. (Nov 1999). "Malignant epithelial odontogenic tumors.". Semin Diagn Pathol 16 (4): 317-24. PMID 10587275.
- ↑ URL: http://www.pathconsultddx.com/pathCon/diagnosis?pii=S1559-8675%2806%2970616-7. Accessed on: March 9, 2010.