Difference between revisions of "Pineal gland"
Jensflorian (talk | contribs) (→(PTPR)) |
(→General: DICER1) |
||
| Line 146: | Line 146: | ||
*Males > females. | *Males > females. | ||
*Children & young adults. | *Children & young adults. | ||
*Corresponds to WHO IV (ICD-O: 9362/3) | *Corresponds to WHO IV (ICD-O: 9362/3). | ||
*May be a manifestation of the [[DICER1 syndrome]]. | |||
===Microscopic=== | ===Microscopic=== | ||
Revision as of 20:32, 21 August 2018
The pineal gland is thingy that is most noted for the fact that it calcifies with age.
Normal histology
- Cellular.
Overview
Non-neoplastic:
- Cysts
Tumours:[1]
- Primary pineal tumours ~15% of (pineal) tumours - benign to malignant:[2]
- Pineocytoma.
- Pineal parenchymal tumor of intermediate differentiation.
- Pineoblastoma.
- Germ cell tumours:
- Germinoma ~ 50% of (pineal) tumours.
- Teratoma ~ 15% of tumours.
- Choriocarcinoma ~ 5% of tumours.
- Others:
- Direct invasion/extension from surrounding structures (astrocytomas).
- Metastases.
- Lipomas.
- Meningiomas.
Pineal gland cyst

Pineal gland cyst found at autopsy. (WC/Marvin101)
Pineal gland cyst. HE, low mag. (WC/jensflorian)
Pineal gland cyst. HE, higher mag. (WC/jensflorian)



Pineocytoma
General
- Benign tumour of the pineal gland.
- WHO Grade I.
Microscopic
Features:
- Cytologically benign cells (uniform size of nuclei, regular nuclear membrane, light chromatin).
- Pineocytomatous/neurocytic rosette = (irregular) rosette with a large meshwork of fibers (neuropil) at the centre.[5]
- Similar to Homer-Wright rosette... but:
- Neuropil centre is larger in pineocytoma.
- Edge of neuropil meshwork irregular.
- Similar to Homer-Wright rosette... but:
Notes:
- Rosette = circular/flower-like arrangement of cells.
Images
Pineocytoma - intermed. mag. (WC)
Pineocytoma - high mag. (WC)
Pineocytoma - very high mag. (WC)



IHC
- Synaptophysin +ve.
- Chromogranin A -ve.
- NSE +ve (cytoplasmic + nuclear).[6]
- GFAP -ve.
- +ve in gliomas.
- PLAP -ve.
- Usu. +ve in germ cell tumours.
- Ki-67.
Another ref.:[7]
Pineal parenchymal tumor of intermediate differentiation
General
- 20% of all pineal tumors.
- Affects all ages.
- ICD-O: 9362/3
- No WHO grade yet, clinical behaviour corresponds to grade II/III[8]
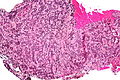
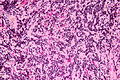
Microscopic
Features:[9]
- High cellularity.
- Mild to moderate atypia.
- Mitoses.
- Usually no pinecytomatous rosettes.
- High pleomorphism possible.
Images:
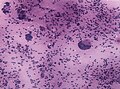
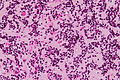
PPID, Smear with plemorphic cells. (WC/jensflorian)
PPID, HE intermed. mag. (WC/jensflorian)
PPID, HE higher mag. (WC/jensflorian)
PPID, HE, rosette-like growth pattern. (WC/jensflorian)




Papillary tumour of pineal region (PTPR)
General
- Very rare neuoepithelial tumor of adults.
- Proposed ICD-O: 9395/3
- No WHO grade yet, clinical behaviour corresponds to grade II/III[10]
Gross:
- Well circumscribed.
- Can be quite large (2-4cm).
- Macroscopy mimics pineocytoma.
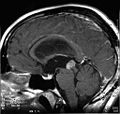
PTPR MRI scan (WC/marvin101)

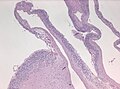
Microscopic
Features:[11]
- Papillary growth pattern.
- Dense areas exhibit ependymal features.
- Clear, vacuolated cytoplasm.
- Rosettes.
- Round to oval nuclei.
- Mitoses (0-10/HPF).
- Necroses.
- Hyalinized vessels.
IHC
- +ve for keratins (KL1, AE1/AE3, Cam5.2, CK18).
- GFAP and Synaptophysin focally +ve.
- S100+ve.
- EMA mostly -ve.
- NF and Kir 7.1-ve.
DDx: Ependymoma.
Images:
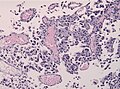
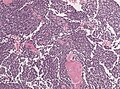
PTPR H&E stain (WC/jensflorian)
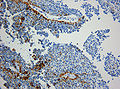
PTPR CK KL1 (WC/marvin101)
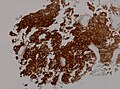
PTPR CK18 IHC (WC/jensflorian)
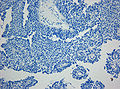
PTPR EMA IHC (WC/marvin101)

PTPR Kir 7.1 IHC (WC/marvin101)





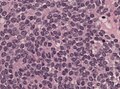
Pineoblastoma
General
- Rare.
- Malignant.
- Males > females.
- Children & young adults.
- Corresponds to WHO IV (ICD-O: 9362/3).
- May be a manifestation of the DICER1 syndrome.
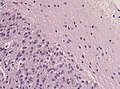
Microscopic
Features:
- Hypercellular.
- Mitoses.
- Nuclear atypia.
- Homer-wright & Flexner-Winterstein rosettes
- Fleurettes.
IHC
- GFAP -ve/+ve.
- NF+ve.
- Synaptophysin+ve
- MIB-1: high.
DDx:
- Glioblastoma, small cell variant.
- Small round cell tumors.
Images:
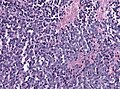
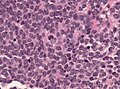
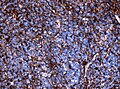
Pineoblastoma H&E (WC/jensflorian)
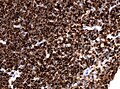
Neurofilament IHC in Pineoblastoma (WC/jensflorian)
GFAP IHC in Pineoblastoma (WC/jensflorian)



See also
References
- ↑ Gaillard F, Jones J (October 2010). "Masses of the pineal region: clinical presentation and radiographic features". Postgrad Med J 86 (1020): 597–607. doi:10.1136/pgmj.2009.087460. PMID 20971711.
- ↑ Smith AB, Rushing EJ, Smirniotopoulos JG (November 2010). "From the archives of the AFIP: lesions of the pineal region: radiologic-pathologic correlation". Radiographics 30 (7): 2001–20. doi:10.1148/rg.307105131. PMID 21057132.
- ↑ Pu, Y.; Mahankali, S.; Hou, J.; Li, J.; Lancaster, JL.; Gao, JH.; Appelbaum, DE.; Fox, PT. (Oct 2007). "High prevalence of pineal cysts in healthy adults demonstrated by high-resolution, noncontrast brain MR imaging.". AJNR Am J Neuroradiol 28 (9): 1706-9. doi:10.3174/ajnr.A0656. PMID 17885233.
- ↑ Mena, H.; Armonda, RA.; Ribas, JL.; Ondra, SL.; Rushing, EJ. (Oct 1997). "Nonneoplastic pineal cysts: a clinicopathologic study of twenty-one cases.". Ann Diagn Pathol 1 (1): 11-8. PMID 9869821.
- ↑ Wippold FJ, Perry A (March 2006). "Neuropathology for the neuroradiologist: rosettes and pseudorosettes". AJNR Am J Neuroradiol 27 (3): 488–92. PMID 16551982.
- ↑ URL: http://path.upmc.edu/cases/case157/dx.html. Accessed on: 9 December 2010.
- ↑ URL: http://www.springerlink.com/content/k4v88n6h6jknhp2t/fulltext.pdf. Accessed on: 9 December 2010.
- ↑ Jouvet, A.; Saint-Pierre, G.; Fauchon, F.; Privat, K.; Bouffet, E.; Ruchoux, MM.; Chauveinc, L.; Fèvre-Montange, M. (Jan 2000). "Pineal parenchymal tumors: a correlation of histological features with prognosis in 66 cases.". Brain Pathol 10 (1): 49-60. PMID 10668895.
- ↑ Fèvre-Montange, M.; Szathmari, A.; Champier, J.; Mokhtari, K.; Chrétien, F.; Coulon, A.; Figarella-Branger, D.; Polivka, M. et al. (Jul 2008). "Pineocytoma and pineal parenchymal tumors of intermediate differentiation presenting cytologic pleomorphism: a multicenter study.". Brain Pathol 18 (3): 354-9. doi:10.1111/j.1750-3639.2008.00128.x. PMID 18371183.
- ↑ Fèvre-Montange, M.; Hasselblatt, M.; Figarella-Branger, D.; Chauveinc, L.; Champier, J.; Saint-Pierre, G.; Taillandier, L.; Coulon, A. et al. (Oct 2006). "Prognosis and histopathologic features in papillary tumors of the pineal region: a retrospective multicenter study of 31 cases.". J Neuropathol Exp Neurol 65 (10): 1004-11. doi:10.1097/01.jnen.0000240462.80263.13. PMID 17021405.
- ↑ Heim, S.; Beschorner, R.; Mittelbronn, M.; Keyvani, K.; Riemenschneider, MJ.; Vajtai, I.; Hartmann, C.; Acker, T. et al. (Jan 2014). "Increased mitotic and proliferative activity are associated with worse prognosis in papillary tumors of the pineal region.". Am J Surg Pathol 38 (1): 106-10. doi:10.1097/PAS.0b013e31829e492d. PMID 24121176.