Difference between revisions of "Neuroendocrine neoplasms"
Jump to navigation
Jump to search
(→Stomach: more) |
|||
| Line 66: | Line 66: | ||
===Stomach=== | ===Stomach=== | ||
Divided into four types: | Divided into four types:<ref>URL: [http://www.cap.org/apps/docs/committees/cancer/cancer_protocols/2011/StomachNET_11protocol.pdf http://www.cap.org/apps/docs/committees/cancer/cancer_protocols/2011/StomachNET_11protocol.pdf]. Accessed on: 29 March 2012.</ref> | ||
*Type I. | *Type I. | ||
**Chronic atrophic gastritis - usually autoimmune gastritis. | **Chronic atrophic gastritis - usually autoimmune gastritis. | ||
**Hypochlorhydia. | **Hypochlorhydia. | ||
**Good prognosis. | |||
*Type II. | *Type II. | ||
**[[Zollinger-Ellison syndrome]] | **[[Zollinger-Ellison syndrome]]. | ||
***Often [[MEN 1]] - may be multifocal. | |||
**Hyperchlorhydia, pancreatic ''or'' duodenal NET secreting gastrin (gastrinoma). | **Hyperchlorhydia, pancreatic ''or'' duodenal NET secreting gastrin (gastrinoma). | ||
**Rare. | |||
**Poor prognosis. | |||
*Type III. | *Type III. | ||
**Usually solitary. | |||
**Sporadic. | |||
**Normal gastrin. | **Normal gastrin. | ||
**Aggressive. | **Aggressive behaviour if > 2.0 cm. | ||
*Type IV. | *Type IV. | ||
**Elevated gastrin due to parietal cell dysfunction. | **Elevated gastrin due to parietal cell dysfunction. | ||
**Extremely rare. | **Extremely rare. | ||
**Usually metastases at time of diagnosis. | |||
===Pancreatic=== | ===Pancreatic=== | ||
Revision as of 16:30, 29 March 2012
Neuroendocrine neoplasms, also neuroendocrine tumours, are a group of tumours whose behaviour varies from benign to malignant and are found in may different sites.
These tumours arise from epithelium; thus, malignant tumours in this group are referred to as neuroendocrine carcinomas.
Use of the term carcinoid
Use of the term carcinoid is discouraged (in pathology reports), in the context of gastrointestinal pathology.[1][2][3]
The term is still used for neuroendocrine tumours of the lung - see carcinoid tumours.
Carcinoid syndrome
Pathophysiology
- Neuroendocrine tumour -> hormone secretion (5-hydroxytryptamine + others).[4]
Clinical
Features:[4]
- Diarrhea, flushing and wheezing.
Pathologic findings
Classic pathologic finding:[4]
- Fibrosis of cardiac valves (tricuspid and pulmonary).
- Result TIPS = tricuspid insufficiency pulmonary stenosis.
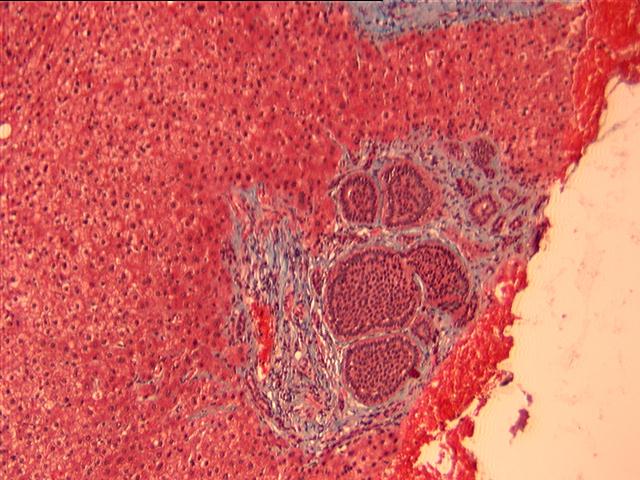
Microscopic - generic
Features:
- Nests of cells - with fibrous stroma in between.
- May have a trabecular architecture.
- Stippled chromatin AKA salt-and-pepper chromatin, coarse chromatin.
- Classically subepithelial/mural.
DDx:
Images:
- WC:
- www:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Site specific
Lung
Main article: Lung_tumours#Neuroendocrine_tumours
Gastrointestinal tract
Main article: Duodenum#Neuroendocrine_tumours
WHO classification for digestive NET
Subtypes:[6]
- Neuroendocrine tumour G1.
- Neuroendocrine tumour G2.
- Neuroendocrine carcinoma, small cell type.
- Neuroendocrine carcinoma, large cell type.
- Mixed adenoneuroendocrine carcinoma.
Grading
Grading of NETs:[7]
- Grade 1 (G1): < 2 mitoses/2 mm^2 or < 3% Ki-67.
- Grade 2 (G2): > 2 mitoses/2 mm^2 or > 3% Ki-67 and < 20 mitoses/2 mm^2 or < 20% Ki-67.
- Grade 3 (G3): > 20 mitoses/2 mm^2 or > 20% Ki-67.
Notes:
- Neuroendocrine carcinomas are G3 by definition.
Stomach
Divided into four types:[8]
- Type I.
- Chronic atrophic gastritis - usually autoimmune gastritis.
- Hypochlorhydia.
- Good prognosis.
- Type II.
- Zollinger-Ellison syndrome.
- Often MEN 1 - may be multifocal.
- Hyperchlorhydia, pancreatic or duodenal NET secreting gastrin (gastrinoma).
- Rare.
- Poor prognosis.
- Zollinger-Ellison syndrome.
- Type III.
- Usually solitary.
- Sporadic.
- Normal gastrin.
- Aggressive behaviour if > 2.0 cm.
- Type IV.
- Elevated gastrin due to parietal cell dysfunction.
- Extremely rare.
- Usually metastases at time of diagnosis.
Pancreatic
Main article: Pancreatic neuroendocrine tumour
See also
References
- ↑ Chetty, R. (Apr 2008). "Requiem for the term 'carcinoid tumour' in the gastrointestinal tract?". Can J Gastroenterol 22 (4): 357-8. PMID 18414708.
- ↑ Klöppel, G.; Perren, A.; Heitz, PU. (Apr 2004). "The gastroenteropancreatic neuroendocrine cell system and its tumors: the WHO classification.". Ann N Y Acad Sci 1014: 13-27. PMID 15153416.
- ↑ Klöppel G (July 2003). "[Neuroendocrine tumors of the gastrointestinal tract]" (in German). Pathologe 24 (4): 287–96. doi:10.1007/s00292-003-0636-7. PMID 14513276.
- ↑ 4.0 4.1 4.2 Druce, M.; Rockall, A.; Grossman, AB. (May 2009). "Fibrosis and carcinoid syndrome: from causation to future therapy.". Nat Rev Endocrinol 5 (5): 276-83. doi:10.1038/nrendo.2009.51. PMID 19444261.
- ↑ URL: [http://path.upmc.edu/cases/case7.html http://path.upmc.edu/cases/case7.html}. Accessed on: 17 December 2011.
- ↑ Scoazec, JY.; Couvelard, A. (Apr 2011). "[The new WHO classification of digestive neuroendocrine tumors].". Ann Pathol 31 (2): 88-92. doi:10.1016/j.annpat.2011.01.001. PMID 21601112.
- ↑ Volante, M.; Righi, L.; Berruti, A.; Rindi, G.; Papotti, M. (Apr 2011). "The pathological diagnosis of neuroendocrine tumors: common questions and tentative answers.". Virchows Arch 458 (4): 393-402. doi:10.1007/s00428-011-1060-7. PMID 21344263.
- ↑ URL: http://www.cap.org/apps/docs/committees/cancer/cancer_protocols/2011/StomachNET_11protocol.pdf. Accessed on: 29 March 2012.