Difference between revisions of "Acute infectious pneumonia"
Jump to navigation
Jump to search
(split out) |
|||
| (One intermediate revision by the same user not shown) | |||
| Line 2: | Line 2: | ||
==General== | ==General== | ||
* | Clinical features: | ||
*[[Dyspnea]]. | |||
*Chest pain. | |||
*Fever. | |||
It is seen by pathologists at [[autopsy]] from time-to-time, and in advanced [[lung cancer]]. | |||
===Etiology=== | |||
Most common cause: | Most common cause: | ||
*''Streptococcus pneumoniae''.<ref name=Ref_PBoD8_711>{{Ref PBoD8|711}}</ref> | *''Streptococcus pneumoniae''.<ref name=Ref_PBoD8_711>{{Ref PBoD8|711}}</ref> | ||
| Line 67: | Line 73: | ||
==See also== | ==See also== | ||
*[[Pneumonia]]. | *[[Pneumonia]]. | ||
*[[Acute pneumonia]]. | |||
==References== | ==References== | ||
Latest revision as of 16:01, 13 February 2016
Acute infectious pneumonia is a common type of pneumonia. It is usually diagnosed clinically and uncommonly biopsied.
General
Clinical features:
- Dyspnea.
- Chest pain.
- Fever.
It is seen by pathologists at autopsy from time-to-time, and in advanced lung cancer.
Etiology
Most common cause:
- Streptococcus pneumoniae.[1]
The top three community acquired (acute) pneumonia:[2]
- Streptococcuc pneumonia.
- Haemophilus influenzae.
- Moraxella catarrhalis.
Other community acquired pneumonia:[1]
- S. aureus.
- Legionaella pneumophila.
- Klebsiella pneumoniae.
- Pseudomonas.
Hospital-acquired pneumonia:[1]
- Gram-negative rods.
- Staphylococcus aureus.
Radiologic correlate
- Air space disease.
Gross pathology
- Consolidation (the lung parenchyma is firm) - best appreciated by running a finger over the cut surface of the lung with a small-to-moderate amount of pressure.
Bronchopneumonia:
- Classically yellow-white centered on the bronchi.[3]
Lobar pneumnia is classically described in four stages:[4][5]
- Congestion - day 1-2.
- Red hepatization - day 2-4.
- Gray hepatization - day 4-6.
- Resolution - day 6+.
Note:
- The stages of lobar pneumonia is considered more-or-less historical. In the age of antibiotics, lobar pneumonia is uncommon.
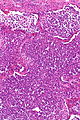
Microscopic
Features:
- Alveoli packed with PMNs.
- +/-Clusters of bacteria - small dots or rods.
- +/-Abscess formation.
DDx:
- Aspiration pneumonia - aspirated material, usually lack microorganisms.
Images

Normal alveoli & pneumonia. (WC)


AP - low mag. (WC)

AP - intermed. mag. (WC)
AP - intermed. mag. (WC)

AP - high mag. (WC)

AP - very high mag. (WC)





Stains
- Gram stain -- to type the bacteria.
See also
References
- ↑ 1.0 1.1 1.2 Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 711. ISBN 978-1416031215.
- ↑ Nicolau, D. (Sep 2002). "Clinical and economic implications of antimicrobial resistance for the management of community-acquired respiratory tract infections.". J Antimicrob Chemother 50 Suppl S1: 61-70. PMID 12239229.
- ↑ Rose, Alan G. (2008). Atlas of Gross Pathology with Histologic Correlation (1st ed.). Cambridge University Press. pp. 93. ISBN 978-0521868792.
- ↑ Rose, Alan G. (2008). Atlas of Gross Pathology with Histologic Correlation (1st ed.). Cambridge University Press. pp. 92. ISBN 978-0521868792.
- ↑ URL: http://www.histopathology-india.net/Lobar_Pneumonia.htm. Accessed on: 27 February 2012.
- ↑ Rose, Alan G. (2008). Atlas of Gross Pathology with Histologic Correlation (1st ed.). Cambridge University Press. pp. 95. ISBN 978-0521868792.