Difference between revisions of "Hereditary hemochromatosis"
(→Stains) |
(→Images: Added case with cirrhosis) |
||
| (3 intermediate revisions by 2 users not shown) | |||
| Line 42: | Line 42: | ||
www: | www: | ||
*[http://path.upmc.edu/cases/case77/path.html Hemochromatosis (upmc.edu)]. | *[http://path.upmc.edu/cases/case77/path.html Hemochromatosis (upmc.edu)]. | ||
{| | |||
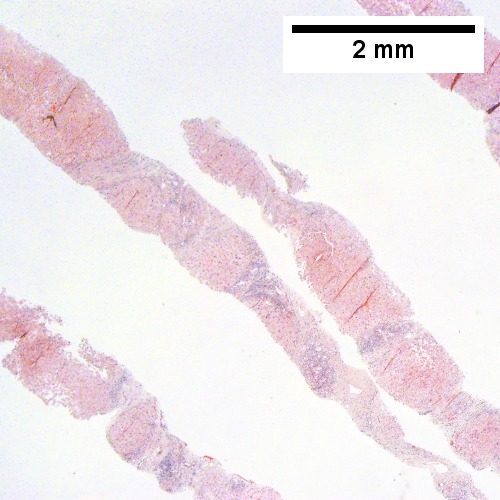
[[File:1 Iron 1 680x512px.tif|Trichrome shows thin fibrous bands (20X).]] | |||
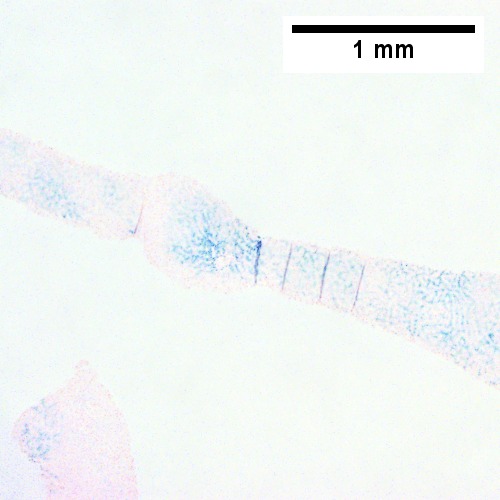
[[File:2 Iron 1 680x512px.tif|Iron stain shows dense iron deposition (40X).]] | |||
|- | |||
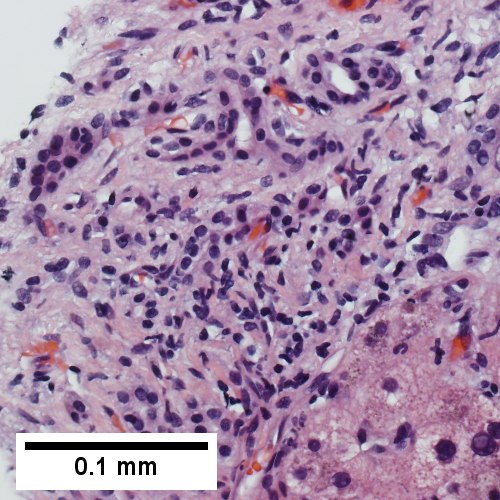
[[File:3 Iron 1 680x512px.tif|At high power, a modest inflammatory infiltrate accompanies proliferating bile ductules; no piecemeal necrosis (400X)]] | |||
[[File:4 Iron 1 1360x1024px.tif|Reticulin stain with regenerative findings, cords with two nuclei thickness, hepatic acini (400X, higher pixel photo)]] | |||
|} | |||
Hemochromatosis with bridging fibrosis. | |||
Trichrome shows thin fibrous bands (Row 1 Left 20X). Iron stain shows dense iron deposition (Row 1 Right 40X). At high power, a modest inflammatory infiltrate accompanies proliferating bile ductules; no piecemeal necrosis (Row 2 Left 400X). Reticulin stain with regenerative findings, cords with two nuclei thickness, hepatic acini (Row 2 right 400X, higher pixel photo). | |||
{| | |||
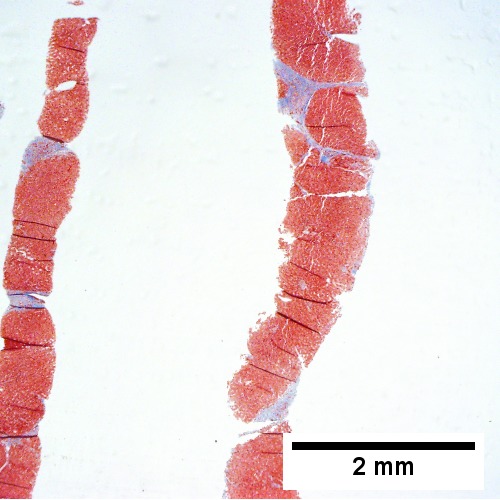
[[File:1 Iron 2 680x512px.tif|Fibrous bands dissect hepatocyte nodules (Row 1 Left 20X).]] | |||
[[File:2 Iron 2 680x512px.tif|Iron stain shows 4+ iron, identifiable at the lowest magnification, as well by naked eye (Row 1 Right 20X)]] | |||
<br> | |||
[[File:3 Iron 2 680x512px.tif|This nodule has occasionally enlarged nuclei, which should not be considered dysplasia in and of itself. Note associated relatively inflammation free band with proliferated bile ductules. (Row 2 Left 400X).]] | |||
[[File:4 Iron 2 680x512px.tif|Reticulin stain shows two cell thick regenerative cords with sinusoidal black lines lacking orientation (Row 2 Right 400X).]] | |||
|} | |||
Hemochromatosis with cirrhosis.. | |||
Fibrous bands dissect hepatocyte nodules (Row 1 Left 20X). Iron stain shows 4+ iron, identifiable at the lowest magnification, as well by naked eye (Row 1 Right 20X) This nodule has occasionally enlarged nuclei, which should not be considered dysplasia in and of itself. Note associated relatively inflammation free band with proliferated bile ductules. (Row 2 Left 400X). Reticulin stain shows two cell thick regenerative cords with sinusoidal black lines lacking orientation (Row 2 Right 400X). | |||
==Stains== | ==Stains== | ||
Iron stain +ve -- '''important'''. | Iron stain +ve -- '''important'''. | ||
| Line 47: | Line 66: | ||
**Must be separated from ''siderosis'' -- iron in Kupffer cells. | **Must be separated from ''siderosis'' -- iron in Kupffer cells. | ||
Grading | ===Grading=== | ||
The quantity of iron is scored as follows: | |||
*0 = none. | *0 = none. | ||
*1: only at high power. | *1: only at high power. | ||
Latest revision as of 14:35, 29 August 2016
Hereditary hemochromatosis, abbreviated HH, is a genetic (autosomal dominant inherited) cause of iron deposition.
Secondary causes of hemochromatosis are dealt with in secondary hemochromatosis.
General
Epidemiology:
- Genetic defect - HFE gene.[1]
- Onset in males earlier than females (due to menses).
- Mutation thought to confer survival advantage - several theories (increased resistance to TB, S. typhi vs. decreased iron deficiency/increased iron absorption).[2]
Associated pathology (mnemonic: hemochromatosis can cause deposits anywhere):[3][4]
- Hypogonadism.
- Cirrhosis and HCC.
- Cardiomyopathy - DCM (esp. with his63asp mutation),[5] may be RCM.
- Diabetes mellitus (bronze diabetes).
- Arthropathy.[6]
Pathophysiology:
- Iron overload -> cirrhosis.
Microscopic
Features:
- Periportal iron deposition (early).
- Late stage disease has diffuse iron deposition.
- Brown granular - may vaguely look like lipofuscin on H&E.
Notes:
- Iron in the bile ducts and endothelium used to be though specific of hereditary hemochromatosis.[7]
- It is now thought to just reflect the severity of iron deposition, i.e. if the bile ducts and endothelium have iron - it is severe.
DDx - secondary hemochromatosis:
- Myelodysplastic syndrome.
- Chronic hemolysis.
- Alcoholic liver disease; iron deposition common in cirrhosis.
Images
Hemosiderosis - iron stain. (WC)

www:
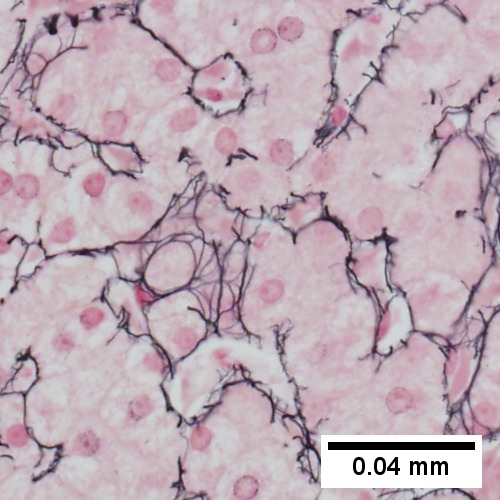
Hemochromatosis with bridging fibrosis. Trichrome shows thin fibrous bands (Row 1 Left 20X). Iron stain shows dense iron deposition (Row 1 Right 40X). At high power, a modest inflammatory infiltrate accompanies proliferating bile ductules; no piecemeal necrosis (Row 2 Left 400X). Reticulin stain with regenerative findings, cords with two nuclei thickness, hepatic acini (Row 2 right 400X, higher pixel photo).
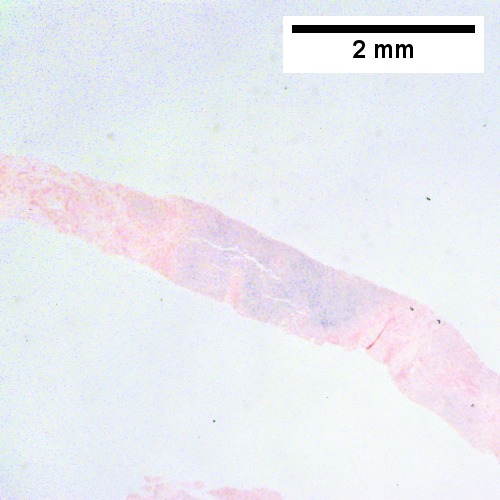

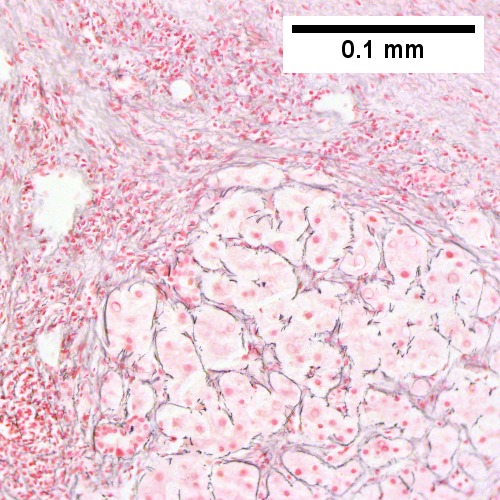
Hemochromatosis with cirrhosis.. Fibrous bands dissect hepatocyte nodules (Row 1 Left 20X). Iron stain shows 4+ iron, identifiable at the lowest magnification, as well by naked eye (Row 1 Right 20X) This nodule has occasionally enlarged nuclei, which should not be considered dysplasia in and of itself. Note associated relatively inflammation free band with proliferated bile ductules. (Row 2 Left 400X). Reticulin stain shows two cell thick regenerative cords with sinusoidal black lines lacking orientation (Row 2 Right 400X).
Stains
Iron stain +ve -- important.
- Light blue haze is not enough.
- Must be separated from siderosis -- iron in Kupffer cells.
Grading
The quantity of iron is scored as follows:
- 0 = none.
- 1: only at high power.
- 2: at medium power.
- 3: at lowest power.
- 4: seen without microscope.
Molecular
- PCR - diagnostic - see molecular pathology tests.
See also
References
- ↑ 1.0 1.1 Online 'Mendelian Inheritance in Man' (OMIM) 613609
- ↑ 2.0 2.1 Weinberg ED (2008). "Survival advantage of the hemochromatosis C282Y mutation". Perspect. Biol. Med. 51 (1): 98-102. doi:10.1353/pbm.2008.0001. PMID 18192769.
- ↑ URL: http://en.wikibooks.org/wiki/USMLE_Step_2_Review. Accessed on: 15 March 2012.
- ↑ Fix, OK.; Kowdley, KV. (Dec 2008). "Hereditary hemochromatosis.". Minerva Med 99 (6): 605-17. PMID 19034258.
- ↑ Mahon, NG.; Coonar, AS.; Jeffery, S.; Coccolo, F.; Akiyu, J.; Zal, B.; Houlston, R.; Levin, GE. et al. (Nov 2000). "Haemochromatosis gene mutations in idiopathic dilated cardiomyopathy.". Heart 84 (5): 541-7. PMID 11040018.
- ↑ von Kempis, J. (Jan 2001). "Arthropathy in hereditary hemochromatosis.". Curr Opin Rheumatol 13 (1): 80-3. PMID 11148720.
- ↑ MG. 17 September 2009.