Difference between revisions of "Typical carcinoid lung tumour"
Jump to navigation
Jump to search
(→IHC) |
|||
| (26 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
{{ Infobox diagnosis | |||
| Name = {{PAGENAME}} | |||
| Image = Lung_carcinoid_-_high_mag.jpg | |||
| Width = | |||
| Caption = Lung carcinoid. [[H&E stain]]. | |||
| Synonyms = lung carcinoid | |||
| Micro = stippled chromatin, usually nested architecture, no necrosis, low mitotic rate (see below) | |||
| Subtypes = | |||
| LMDDx = [[atypical carcinoid lung tumour]], [[pulmonary carcinoid tumourlet]], [[lung adenocarcinoma]] | |||
| Stains = | |||
| IHC = Ki-67 ~2% (0-7%), TTF-1 +ve/-ve, CK7 +ve/-ve, CK20 -ve | |||
| EM = | |||
| Molecular = | |||
| IF = | |||
| Gross = well-circumscribed, solid, >=5 mm (definition) | |||
| Grossing = | |||
| Site = [[lung]] - see ''[[lung tumours]]'' | |||
| Assdx = | |||
| Syndromes = [[diffuse idiopathic pulmonary neuroendocrine cell hyperplasia]] | |||
| Clinicalhx = | |||
| Signs = | |||
| Symptoms = +/-cough, +/-hemoptysis | |||
| Prevalence = not common | |||
| Bloodwork = | |||
| Rads = usually central (85% of cases), well-circumscribed, solid | |||
| Endoscopy = | |||
| Prognosis = benign | |||
| Other = | |||
| ClinDDx = other [[lung tumours]], [[lung metastases]] (esp. when multiple) | |||
| Tx = excision to exclude other types of lung tumours & treat symptoms | |||
}} | |||
'''Typical carcinoid lung tumour''', also '''lung carcinoid''' and '''carcinoid tumour of the lung''', is a benign [[lung tumour]], that is excised to exclude [[malignancy]]. | '''Typical carcinoid lung tumour''', also '''lung carcinoid''' and '''carcinoid tumour of the lung''', is a benign [[lung tumour]], that is excised to exclude [[malignancy]]. | ||
==General== | ==General== | ||
*Approximately 80% of lung carcinoids.<ref name=pmid20888248>{{Cite journal | last1 = Naalsund | first1 = A. | last2 = Rostad | first2 = H. | last3 = Strøm | first3 = EH. | last4 = Lund | first4 = MB. | last5 = Strand | first5 = TE. | title = Carcinoid lung tumors--incidence, treatment and outcomes: a population-based study. | journal = Eur J Cardiothorac Surg | volume = 39 | issue = 4 | pages = 565-9 | month = Apr | year = 2011 | doi = 10.1016/j.ejcts.2010.08.036 | PMID = 20888248 }}</ref> | *Approximately 80% of lung carcinoids.<ref name=pmid20888248>{{Cite journal | last1 = Naalsund | first1 = A. | last2 = Rostad | first2 = H. | last3 = Strøm | first3 = EH. | last4 = Lund | first4 = MB. | last5 = Strand | first5 = TE. | title = Carcinoid lung tumors--incidence, treatment and outcomes: a population-based study. | journal = Eur J Cardiothorac Surg | volume = 39 | issue = 4 | pages = 565-9 | month = Apr | year = 2011 | doi = 10.1016/j.ejcts.2010.08.036 | PMID = 20888248 }}</ref> | ||
*May be multiple.<ref name=pmid356600>{{Cite journal | last1 = Miller | first1 = MA. | last2 = Mark | first2 = GJ. | last3 = Kanarek | first3 = D. | title = Multiple peripheral pulmonary carcinoids and tumorlets of carcinoid type, with restrictive and obstructive lung disease. | journal = Am J Med | volume = 65 | issue = 2 | pages = 373-8 | month = Aug | year = 1978 | doi = | PMID = 356600 }}</ref> | |||
**Can mimicking metastatic disease.<ref name=pmid17400673>{{Cite journal | last1 = Aubry | first1 = MC. | last2 = Thomas | first2 = CF. | last3 = Jett | first3 = JR. | last4 = Swensen | first4 = SJ. | last5 = Myers | first5 = JL. | title = Significance of multiple carcinoid tumors and tumorlets in surgical lung specimens: analysis of 28 patients. | journal = Chest | volume = 131 | issue = 6 | pages = 1635-43 | month = Jun | year = 2007 | doi = 10.1378/chest.06-2788 | PMID = 17400673 }}</ref> | |||
**Often re-occur - but long term survival good. | |||
*Can be seen in the context of [[diffuse idiopathic pulmonary neuroendocrine cell hyperplasia]] (DIPNECH).<ref name=pmid26104490>{{Cite journal | last1 = Wirtschafter | first1 = E. | last2 = Walts | first2 = AE. | last3 = Liu | first3 = ST. | last4 = Marchevsky | first4 = AM. | title = Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia of the Lung (DIPNECH): Current Best Evidence. | journal = Lung | volume = | issue = | pages = | month = Jun | year = 2015 | doi = 10.1007/s00408-015-9755-1 | PMID = 26104490 }}</ref><ref name=pmid26112453>{{Cite journal | last1 = Chauhan | first1 = A. | last2 = Ramirez | first2 = RA. | title = Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia (DIPNECH) and the Role of Somatostatin analogs: A Case Series. | journal = Lung | volume = | issue = | pages = | month = Jun | year = 2015 | doi = 10.1007/s00408-015-9754-2 | PMID = 26112453 }}</ref> | |||
*A common primary lung tumour in children.<ref name=pmid26971789>{{Cite journal | last1 = Giuseppucci | first1 = C. | last2 = Reusmann | first2 = A. | last3 = Giubergia | first3 = V. | last4 = Barrias | first4 = C. | last5 = Krüger | first5 = A. | last6 = Siminovich | first6 = M. | last7 = Botto | first7 = H. | last8 = Cadario | first8 = M. | last9 = Boglione | first9 = M. | title = Primary lung tumors in children: 24 years of experience at a referral center. | journal = Pediatr Surg Int | volume = 32 | issue = 5 | pages = 451-7 | month = May | year = 2016 | doi = 10.1007/s00383-016-3884-3 | PMID = 26971789 }} | |||
</ref> | |||
**Most common lung tumour in children: metastasis (80-85% of lung tumours in children<ref name=pmid>{{Cite journal | last1 = Dishop | first1 = MK. | last2 = Kuruvilla | first2 = S. | title = Primary and metastatic lung tumors in the pediatric population: a review and 25-year experience at a large children's hospital. | journal = Arch Pathol Lab Med | volume = 132 | issue = 7 | pages = 1079-103 | month = Jul | year = 2008 | doi = 10.1043/1543-2165(2008)132[1079:PAMLTI]2.0.CO;2 | PMID = 18605764 }}</ref>). | |||
Presentation:<ref name=pmid16810137>{{Cite journal | last1 = Gungor | first1 = S. | last2 = Damadoglu | first2 = E. | last3 = Aybatli | first3 = A. | last4 = Yilmaz | first4 = A. | last5 = Kir | first5 = A. | last6 = Akkaya | first6 = E. | title = Typical pulmonary carcinoid tumors: presentation and outcome of 24 cases. | journal = Med Sci Monit | volume = 12 | issue = 7 | pages = CR315-8 | month = Jul | year = 2006 | doi = | PMID = 16810137 }}</ref> | Presentation:<ref name=pmid16810137>{{Cite journal | last1 = Gungor | first1 = S. | last2 = Damadoglu | first2 = E. | last3 = Aybatli | first3 = A. | last4 = Yilmaz | first4 = A. | last5 = Kir | first5 = A. | last6 = Akkaya | first6 = E. | title = Typical pulmonary carcinoid tumors: presentation and outcome of 24 cases. | journal = Med Sci Monit | volume = 12 | issue = 7 | pages = CR315-8 | month = Jul | year = 2006 | doi = | PMID = 16810137 }}</ref> | ||
*Cough. | *Cough. | ||
*Hemoptysis. | *Hemoptysis. | ||
Treatment: | |||
*Surgical resection.<ref name=pmid25646366>{{Cite journal | last1 = Caplin | first1 = ME. | last2 = Baudin | first2 = E. | last3 = Ferolla | first3 = P. | last4 = Filosso | first4 = P. | last5 = Garcia-Yuste | first5 = M. | last6 = Lim | first6 = E. | last7 = Oberg | first7 = K. | last8 = Pelosi | first8 = G. | last9 = Perren | first9 = A. | title = Pulmonary neuroendocrine (carcinoid) tumors: European Neuroendocrine Tumor Society expert consensus and recommendations for best practice for typical and atypical pulmonary carcinoids. | journal = Ann Oncol | volume = 26 | issue = 8 | pages = 1604-20 | month = Aug | year = 2015 | doi = 10.1093/annonc/mdv041 | PMID = 25646366 }}</ref> | |||
==Gross== | ==Gross== | ||
| Line 16: | Line 57: | ||
*Nests of cells. | *Nests of cells. | ||
**Stippled chromatin. | **Stippled chromatin. | ||
** | **Scant-to-moderate cytoplasm. | ||
*No necrosis. | *Nuclei round or ellipsoid. | ||
*No necrosis - '''important'''. | |||
*Low mitotic rate. | *Low mitotic rate. | ||
*[[diagnostic size cutoff|Size criterion]]: >= 5 mm.<ref name=pct_ucsf>URL: [http://pathhsw5m54.ucsf.edu/case7/image75.html http://pathhsw5m54.ucsf.edu/case7/image75.html]. Accessed on: 23 January 2012.</ref><ref name=pmid23205296>{{Cite journal | last1 = He | first1 = P. | last2 = Gu | first2 = X. | last3 = Wu | first3 = Q. | last4 = Lin | first4 = Y. | last5 = Gu | first5 = Y. | last6 = He | first6 = J. | title = Pulmonary carcinoid tumorlet without underlying lung disease: analysis of its relationship to fibrosis. | journal = J Thorac Dis | volume = 4 | issue = 6 | pages = 655-8 | month = Dec | year = 2012 | doi = 10.3978/j.issn.2072-1439.2012.06.11 | PMID = 23205296 }}</ref> | *[[diagnostic size cutoff|Size criterion]]: >= 5 mm.<ref name=pct_ucsf>URL: [http://pathhsw5m54.ucsf.edu/case7/image75.html http://pathhsw5m54.ucsf.edu/case7/image75.html]. Accessed on: 23 January 2012.</ref><ref name=pmid23205296>{{Cite journal | last1 = He | first1 = P. | last2 = Gu | first2 = X. | last3 = Wu | first3 = Q. | last4 = Lin | first4 = Y. | last5 = Gu | first5 = Y. | last6 = He | first6 = J. | title = Pulmonary carcinoid tumorlet without underlying lung disease: analysis of its relationship to fibrosis. | journal = J Thorac Dis | volume = 4 | issue = 6 | pages = 655-8 | month = Dec | year = 2012 | doi = 10.3978/j.issn.2072-1439.2012.06.11 | PMID = 23205296 }}</ref> | ||
| Line 25: | Line 67: | ||
*[[Atypical carcinoid lung tumour]]. | *[[Atypical carcinoid lung tumour]]. | ||
*[[Lung adenocarcinoma]].<ref name=pmid22269186>{{Cite journal | last1 = Demirci | first1 = I. | last2 = Herold | first2 = S. | last3 = Kopp | first3 = A. | last4 = Flaßhove | first4 = M. | last5 = Klosterhalfen | first5 = B. | last6 = Janßen | first6 = H. | title = Overdiagnosis of a typical carcinoid tumor as an adenocarcinoma of the lung: a case report and review of the literature. | journal = World J Surg Oncol | volume = 10 | issue = | pages = 19 | month = | year = 2012 | doi = 10.1186/1477-7819-10-19 | PMID = 22269186 }}</ref> | *[[Lung adenocarcinoma]].<ref name=pmid22269186>{{Cite journal | last1 = Demirci | first1 = I. | last2 = Herold | first2 = S. | last3 = Kopp | first3 = A. | last4 = Flaßhove | first4 = M. | last5 = Klosterhalfen | first5 = B. | last6 = Janßen | first6 = H. | title = Overdiagnosis of a typical carcinoid tumor as an adenocarcinoma of the lung: a case report and review of the literature. | journal = World J Surg Oncol | volume = 10 | issue = | pages = 19 | month = | year = 2012 | doi = 10.1186/1477-7819-10-19 | PMID = 22269186 }}</ref> | ||
*[[Pulmonary meningothelial-like nodule]] - usually 1-3 mm, not associated with airway. | |||
===Images=== | ===Images=== | ||
| Line 34: | Line 77: | ||
==IHC== | ==IHC== | ||
Proliferation: | |||
*Ki-67 ~2% (range 0-7%).<ref name=pmid25318848>{{Cite journal | last1 = Liu | first1 = SZ. | last2 = Staats | first2 = PN. | last3 = Goicochea | first3 = L. | last4 = Alexiev | first4 = BA. | last5 = Shah | first5 = N. | last6 = Dixon | first6 = R. | last7 = Burke | first7 = AP. | title = Automated quantification of Ki-67 proliferative index of excised neuroendocrine tumors of the lung. | journal = Diagn Pathol | volume = 9 | issue = | pages = 174 | month = | year = 2014 | doi = 10.1186/s13000-014-0174-z | PMID = 25318848 }}</ref> | *Ki-67 ~2% (range 0-7%).<ref name=pmid25318848>{{Cite journal | last1 = Liu | first1 = SZ. | last2 = Staats | first2 = PN. | last3 = Goicochea | first3 = L. | last4 = Alexiev | first4 = BA. | last5 = Shah | first5 = N. | last6 = Dixon | first6 = R. | last7 = Burke | first7 = AP. | title = Automated quantification of Ki-67 proliferative index of excised neuroendocrine tumors of the lung. | journal = Diagn Pathol | volume = 9 | issue = | pages = 174 | month = | year = 2014 | doi = 10.1186/s13000-014-0174-z | PMID = 25318848 }}</ref> | ||
**[[Atypical lung carcinoid tumour|Atypical carcinoid]] is on average 17% (range 10-26%).<ref name=pmid25318848/> | |||
[[Neuroendocrine markers]]:<ref name=pmid25006841>{{Cite journal | last1 = Sayeg | first1 = Y. | last2 = Sayeg | first2 = M. | last3 = Baum | first3 = RP. | last4 = Kulkarni | first4 = HR. | last5 = Presselt | first5 = N. | last6 = Mäder | first6 = I. | last7 = Kunze | first7 = A. | last8 = Sänger | first8 = J. | last9 = Hörsch | first9 = D. | title = [Pulmonary neuroendocrine neoplasms]. | journal = Pneumologie | volume = 68 | issue = 7 | pages = 456-77 | month = Jul | year = 2014 | doi = 10.1055/s-0034-1365642 | PMID = 25006841 }}</ref><ref name=pmid23676981>{{Cite journal | last1 = Zhu | first1 = L. | last2 = Shen-Tu | first2 = Y. | last3 = Zhang | first3 = J. | last4 = Fan | first4 = X. | title = [Pathological characteristic and clinical management of pulmonary carcinoid]. | journal = Zhongguo Fei Ai Za Zhi | volume = 16 | issue = 5 | pages = 246-51 | month = May | year = 2013 | doi = 10.3779/j.issn.1009-3419.2013.05.06 | PMID = 23676981 }}</ref> | |||
*[[ | *Chromogranin A +ve. | ||
*Synaptophysin +ve. | |||
*[[CD56]] +ve. | |||
**Also +ve in [[pulmonary meningothelial-like nodule]]. | |||
Others: | |||
*[[TTF-1]] +ve/-ve (11 +ve of 16 cases<ref name=pmid11679943/>). | |||
*[[CK7]] +ve/-ve (10 +ve of 16 cases<ref name=pmid11679943>{{Cite journal | last1 = Cai | first1 = YC. | last2 = Banner | first2 = B. | last3 = Glickman | first3 = J. | last4 = Odze | first4 = RD. | title = Cytokeratin 7 and 20 and thyroid transcription factor 1 can help distinguish pulmonary from gastrointestinal carcinoid and pancreatic endocrine tumors. | journal = Hum Pathol | volume = 32 | issue = 10 | pages = 1087-93 | month = Oct | year = 2001 | doi = 10.1053/hupa.2001.28245 | PMID = 11679943 }}</ref>). | |||
*[[CK20]] -ve (0 +ve of 16 cases<ref name=pmid11679943/>). | |||
==Sign out== | ==Sign out== | ||
===Biopsy=== | |||
<pre> | |||
Lung, Left Upper Lobe, Core Biopsy: | |||
- Consistent with typical lung carcinoid. | |||
Comment: | |||
The tumour stains as follow: | |||
POSITIVE: CK7, TTF-1 (very weak, focal), CD56, chromogranin A, synaptophysin. | |||
NEGATIVE: p63. | |||
PROLIFERATION (Ki-67): ~3% of tumour cells. | |||
</pre> | |||
===Excision=== | |||
<pre> | <pre> | ||
A. Lymph Node, Station 2L, Lymphadenectomy: | A. Lymph Node, Station 2L, Lymphadenectomy: | ||
| Line 59: | Line 125: | ||
==See also== | ==See also== | ||
*[[Lung tumours]]. | *[[Lung tumours]]. | ||
*[[Pancreatic neuroendocrine tumour]]. | |||
*[[Gastric neuroendocrine tumour]]. | |||
*[[Neuroendocrine tumours]]. | |||
==References== | ==References== | ||
Latest revision as of 23:40, 17 March 2019
| Typical carcinoid lung tumour | |
|---|---|
| Diagnosis in short | |
 Lung carcinoid. H&E stain. | |
|
| |
| Synonyms | lung carcinoid |
|
| |
| LM | stippled chromatin, usually nested architecture, no necrosis, low mitotic rate (see below) |
| LM DDx | atypical carcinoid lung tumour, pulmonary carcinoid tumourlet, lung adenocarcinoma |
| IHC | Ki-67 ~2% (0-7%), TTF-1 +ve/-ve, CK7 +ve/-ve, CK20 -ve |
| Gross | well-circumscribed, solid, >=5 mm (definition) |
| Site | lung - see lung tumours |
|
| |
| Syndromes | diffuse idiopathic pulmonary neuroendocrine cell hyperplasia |
|
| |
| Symptoms | +/-cough, +/-hemoptysis |
| Prevalence | not common |
| Radiology | usually central (85% of cases), well-circumscribed, solid |
| Prognosis | benign |
| Clin. DDx | other lung tumours, lung metastases (esp. when multiple) |
| Treatment | excision to exclude other types of lung tumours & treat symptoms |
Typical carcinoid lung tumour, also lung carcinoid and carcinoid tumour of the lung, is a benign lung tumour, that is excised to exclude malignancy.
General
- Approximately 80% of lung carcinoids.[1]
- May be multiple.[2]
- Can mimicking metastatic disease.[3]
- Often re-occur - but long term survival good.
- Can be seen in the context of diffuse idiopathic pulmonary neuroendocrine cell hyperplasia (DIPNECH).[4][5]
- A common primary lung tumour in children.[6]
- Most common lung tumour in children: metastasis (80-85% of lung tumours in children[7]).
Presentation:[8]
- Cough.
- Hemoptysis.
Treatment:
- Surgical resection.[9]
Gross
- Well-circumscribed, solid.
- Location - central airways (85%), remainder peripheral.[10]
Microscopic
Features:
- Nests of cells.
- Stippled chromatin.
- Scant-to-moderate cytoplasm.
- Nuclei round or ellipsoid.
- No necrosis - important.
- Low mitotic rate.
- Size criterion: >= 5 mm.[11][12]
DDx:
- Pulmonary carcinoid tumourlet.
- Atypical carcinoid lung tumour.
- Lung adenocarcinoma.[13]
- Pulmonary meningothelial-like nodule - usually 1-3 mm, not associated with airway.
Images
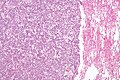
Lung carcinoid - low mag. (WC)
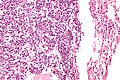
Lung carcinoid - high mag. (WC)
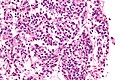
Lung carcinoid - very high mag. (WC)


IHC
Proliferation:
- Ki-67 ~2% (range 0-7%).[14]
- Atypical carcinoid is on average 17% (range 10-26%).[14]
Neuroendocrine markers:[15][16]
- Chromogranin A +ve.
- Synaptophysin +ve.
- CD56 +ve.
- Also +ve in pulmonary meningothelial-like nodule.
Others:
- TTF-1 +ve/-ve (11 +ve of 16 cases[17]).
- CK7 +ve/-ve (10 +ve of 16 cases[17]).
- CK20 -ve (0 +ve of 16 cases[17]).
Sign out
Biopsy
Lung, Left Upper Lobe, Core Biopsy: - Consistent with typical lung carcinoid. Comment: The tumour stains as follow: POSITIVE: CK7, TTF-1 (very weak, focal), CD56, chromogranin A, synaptophysin. NEGATIVE: p63. PROLIFERATION (Ki-67): ~3% of tumour cells.
Excision
A. Lymph Node, Station 2L, Lymphadenectomy: - Lymph node, NEGATIVE for malignancy. B. Lymph Node, Station 4L, Lymphadenectomy: - Lymph node, NEGATIVE for malignancy. C. Lymph Node, Station 11L, Lymphadenectomy: - Lymph node, NEGATIVE for malignancy. D. Lung, Left Upper Lobe, Lobectomy: - Typical carcinoid tumour (12 mm maximal dimension). - Carcinoid tumourlet (2 mm maximal dimension). - Margins clear of tumour. - Please see tumour summary.
See also
- Lung tumours.
- Pancreatic neuroendocrine tumour.
- Gastric neuroendocrine tumour.
- Neuroendocrine tumours.
References
- ↑ Naalsund, A.; Rostad, H.; Strøm, EH.; Lund, MB.; Strand, TE. (Apr 2011). "Carcinoid lung tumors--incidence, treatment and outcomes: a population-based study.". Eur J Cardiothorac Surg 39 (4): 565-9. doi:10.1016/j.ejcts.2010.08.036. PMID 20888248.
- ↑ Miller, MA.; Mark, GJ.; Kanarek, D. (Aug 1978). "Multiple peripheral pulmonary carcinoids and tumorlets of carcinoid type, with restrictive and obstructive lung disease.". Am J Med 65 (2): 373-8. PMID 356600.
- ↑ Aubry, MC.; Thomas, CF.; Jett, JR.; Swensen, SJ.; Myers, JL. (Jun 2007). "Significance of multiple carcinoid tumors and tumorlets in surgical lung specimens: analysis of 28 patients.". Chest 131 (6): 1635-43. doi:10.1378/chest.06-2788. PMID 17400673.
- ↑ Wirtschafter, E.; Walts, AE.; Liu, ST.; Marchevsky, AM. (Jun 2015). "Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia of the Lung (DIPNECH): Current Best Evidence.". Lung. doi:10.1007/s00408-015-9755-1. PMID 26104490.
- ↑ Chauhan, A.; Ramirez, RA. (Jun 2015). "Diffuse Idiopathic Pulmonary Neuroendocrine Cell Hyperplasia (DIPNECH) and the Role of Somatostatin analogs: A Case Series.". Lung. doi:10.1007/s00408-015-9754-2. PMID 26112453.
- ↑ Giuseppucci, C.; Reusmann, A.; Giubergia, V.; Barrias, C.; Krüger, A.; Siminovich, M.; Botto, H.; Cadario, M. et al. (May 2016). "Primary lung tumors in children: 24 years of experience at a referral center.". Pediatr Surg Int 32 (5): 451-7. doi:10.1007/s00383-016-3884-3. PMID 26971789.
- ↑ Dishop, MK.; Kuruvilla, S. (Jul 2008). "Primary and metastatic lung tumors in the pediatric population: a review and 25-year experience at a large children's hospital.". Arch Pathol Lab Med 132 (7): 1079-103. doi:10.1043/1543-2165(2008)132[1079:PAMLTI]2.0.CO;2. PMID 18605764.
- ↑ Gungor, S.; Damadoglu, E.; Aybatli, A.; Yilmaz, A.; Kir, A.; Akkaya, E. (Jul 2006). "Typical pulmonary carcinoid tumors: presentation and outcome of 24 cases.". Med Sci Monit 12 (7): CR315-8. PMID 16810137.
- ↑ Caplin, ME.; Baudin, E.; Ferolla, P.; Filosso, P.; Garcia-Yuste, M.; Lim, E.; Oberg, K.; Pelosi, G. et al. (Aug 2015). "Pulmonary neuroendocrine (carcinoid) tumors: European Neuroendocrine Tumor Society expert consensus and recommendations for best practice for typical and atypical pulmonary carcinoids.". Ann Oncol 26 (8): 1604-20. doi:10.1093/annonc/mdv041. PMID 25646366.
- ↑ Meisinger, QC.; Klein, JS.; Butnor, KJ.; Gentchos, G.; Leavitt, BJ. (Nov 2011). "CT features of peripheral pulmonary carcinoid tumors.". AJR Am J Roentgenol 197 (5): 1073-80. doi:10.2214/AJR.10.5954. PMID 22021498.
- ↑ URL: http://pathhsw5m54.ucsf.edu/case7/image75.html. Accessed on: 23 January 2012.
- ↑ He, P.; Gu, X.; Wu, Q.; Lin, Y.; Gu, Y.; He, J. (Dec 2012). "Pulmonary carcinoid tumorlet without underlying lung disease: analysis of its relationship to fibrosis.". J Thorac Dis 4 (6): 655-8. doi:10.3978/j.issn.2072-1439.2012.06.11. PMID 23205296.
- ↑ Demirci, I.; Herold, S.; Kopp, A.; Flaßhove, M.; Klosterhalfen, B.; Janßen, H. (2012). "Overdiagnosis of a typical carcinoid tumor as an adenocarcinoma of the lung: a case report and review of the literature.". World J Surg Oncol 10: 19. doi:10.1186/1477-7819-10-19. PMID 22269186.
- ↑ 14.0 14.1 Liu, SZ.; Staats, PN.; Goicochea, L.; Alexiev, BA.; Shah, N.; Dixon, R.; Burke, AP. (2014). "Automated quantification of Ki-67 proliferative index of excised neuroendocrine tumors of the lung.". Diagn Pathol 9: 174. doi:10.1186/s13000-014-0174-z. PMID 25318848.
- ↑ Sayeg, Y.; Sayeg, M.; Baum, RP.; Kulkarni, HR.; Presselt, N.; Mäder, I.; Kunze, A.; Sänger, J. et al. (Jul 2014). "[Pulmonary neuroendocrine neoplasms].". Pneumologie 68 (7): 456-77. doi:10.1055/s-0034-1365642. PMID 25006841.
- ↑ Zhu, L.; Shen-Tu, Y.; Zhang, J.; Fan, X. (May 2013). "[Pathological characteristic and clinical management of pulmonary carcinoid].". Zhongguo Fei Ai Za Zhi 16 (5): 246-51. doi:10.3779/j.issn.1009-3419.2013.05.06. PMID 23676981.
- ↑ 17.0 17.1 17.2 Cai, YC.; Banner, B.; Glickman, J.; Odze, RD. (Oct 2001). "Cytokeratin 7 and 20 and thyroid transcription factor 1 can help distinguish pulmonary from gastrointestinal carcinoid and pancreatic endocrine tumors.". Hum Pathol 32 (10): 1087-93. doi:10.1053/hupa.2001.28245. PMID 11679943.