Difference between revisions of "Leydig cell hyperplasia"
Jump to navigation
Jump to search
| (17 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
{{ Infobox diagnosis | |||
| Name = {{PAGENAME}} | |||
| Image = Leydig cell hyperplasia -- low mag.jpg | |||
| Width = | |||
| Caption = Leydig cell hyperplasia. [[H&E stain]]. (WC) | |||
| Synonyms = | |||
| Micro = abundant Leydig cells interspersed between seminiferous tubules with only Sertoli cells, Leydig cells do not displace or compress the seminiferous tubules | |||
| Subtypes = | |||
| LMDDx = [[Leydig cell tumour]], [[testicular adrenal rest tumour]] | |||
| Stains = | |||
| IHC = | |||
| EM = | |||
| Molecular = | |||
| IF = | |||
| Gross = | |||
| Grossing = | |||
| Staging = | |||
| Site = [[testis]], [[ovary]] | |||
| Assdx = | |||
| Syndromes = | |||
| Clinicalhx = | |||
| Signs = | |||
| Symptoms = | |||
| Prevalence = rare | |||
| Bloodwork = | |||
| Rads = hypoechoic lesions on ultrasound, often multiple | |||
| Endoscopy = | |||
| Prognosis = benign | |||
| Other = | |||
| ClinDDx = | |||
| Tx = | |||
}} | |||
'''Leydig cell hyperplasia''' is an uncommon benign [[pathology]] of the [[testis]].<ref name=pmid12540460>{{Cite journal | last1 = Carucci | first1 = LR. | last2 = Tirkes | first2 = AT. | last3 = Pretorius | first3 = ES. | last4 = Genega | first4 = EM. | last5 = Weinstein | first5 = SP. | title = Testicular Leydig's cell hyperplasia: MR imaging and sonographic findings. | journal = AJR Am J Roentgenol | volume = 180 | issue = 2 | pages = 501-3 | month = Feb | year = 2003 | doi = 10.2214/ajr.180.2.1800501 | PMID = 12540460 }}</ref> It may be seen in the [[ovary]]. | '''Leydig cell hyperplasia''' is an uncommon benign [[pathology]] of the [[testis]].<ref name=pmid12540460>{{Cite journal | last1 = Carucci | first1 = LR. | last2 = Tirkes | first2 = AT. | last3 = Pretorius | first3 = ES. | last4 = Genega | first4 = EM. | last5 = Weinstein | first5 = SP. | title = Testicular Leydig's cell hyperplasia: MR imaging and sonographic findings. | journal = AJR Am J Roentgenol | volume = 180 | issue = 2 | pages = 501-3 | month = Feb | year = 2003 | doi = 10.2214/ajr.180.2.1800501 | PMID = 12540460 }}</ref> It may be seen in the [[ovary]]. | ||
==General== | ==General== | ||
* | *Benign. | ||
*Uncommonly seen in isolation by pathology. | |||
A longer list of causes:<ref name=pmid9488073>{{Cite journal | last1 = Naughton | first1 = CK. | last2 = Nadler | first2 = RB. | last3 = Basler | first3 = JW. | last4 = Humphrey | first4 = PA. | title = Leydig cell hyperplasia. | journal = Br J Urol | volume = 81 | issue = 2 | pages = 282-9 | month = Feb | year = 1998 | doi = 10.1046/j.1464-410X.1998.00503.x | PMID = 9488073 }}</ref> | |||
*Congenital (primary). | |||
*Secondary causes: | |||
**Germ cell loss/decrease: | |||
***[[Cryptorchidism]]. | |||
***Advanced age. | |||
**Endocrine-related: | |||
***Adrenal hyperplasia. | |||
***Excess hCG - exogenous or tumour. | |||
Other associations:<ref name=pmid9488073/> | |||
*[[Klinefelter's syndrome]].<ref name=pmid26209412>{{Cite journal | last1 = Sterbis | first1 = J. | last2 = E-Nunu | first2 = T. | title = Leydig cell hyperplasia in the setting of Klinefelter syndrome. | journal = BMJ Case Rep | volume = 2015 | issue = | pages = | month = | year = 2015 | doi = 10.1136/bcr-2015-209805 | PMID = 26209412 }}</ref> | |||
*[[Pernicious anemia]]. | |||
*[[Alcoholism]]. | |||
*Infection - [[syphilis]], [[tuberculosis]]. | |||
==Gross== | ==Gross== | ||
*Unremarkable. | Features: | ||
*Unremarkable gross appearance of parenchyma. (???) | |||
*Normal or small testis. (???) | |||
Note: | Note: | ||
*Hypoechoic lesions on ultrasound.<ref name=pmid26209412/> | *Hypoechoic lesions on ultrasound - often multiple, small.<ref name=pmid26209412/> | ||
==Microscopic== | ==Microscopic== | ||
Features: | Features: | ||
*Abundant Leydig cells interspersed between tubules with only Sertoli cells. | *Abundant Leydig cells interspersed between seminiferous tubules with only Sertoli cells. | ||
**Leydig cells do ''not'' displace or compress the seminiferous tubules. | |||
Note: | |||
*May form nodules up to 6 mm.<ref name=pmid12540460/> | |||
DDx: | DDx: | ||
*[[Leydig cell tumour]]. | *[[Leydig cell tumour]]. | ||
*[[Testicular adrenal rest tumour]]. | |||
===Images=== | |||
<gallery> | |||
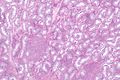
Image: Leydig cell hyperplasia -- very low mag.jpg | LCH - very low mag. (WC) | |||
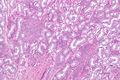
Image: Leydig cell hyperplasia - alt -- very low mag.jpg | LCH - very low mag. (WC) | |||
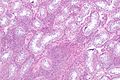
Image: Leydig cell hyperplasia -- low mag.jpg | LCH - low mag. (WC) | |||
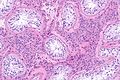
Image: Leydig cell hyperplasia -- intermed mag.jpg | LCH - intermed. mag. (WC) | |||
Image: Leydig cell hyperplasia -- high mag.jpg | LCH - high mag. (WC) | |||
Image: Leydig cell hyperplasia - alt -- high mag.jpg | LCH - high mag. (WC) | |||
</gallery> | |||
==Sign out== | |||
<pre> | |||
Testicle and Cord, Right, Orchitectomy: | |||
- Leydig cell hyperplasia. | |||
- Atrophic testis. | |||
- NEGATIVE for germ cell neoplasia in situ (intratubular germ cell neoplasia). | |||
- NEGATIVE for malignancy. | |||
Comment: | |||
Immunostains confirm the morphologic impression. | |||
The Leydig cells are POSITIVE for inhibin, calretinin and melan A. The section is | |||
NEGATIVE for PLAP and has a benign pattern for D2-40. | |||
</pre> | |||
==See also== | ==See also== | ||
Latest revision as of 11:40, 25 June 2016
| Leydig cell hyperplasia | |
|---|---|
| Diagnosis in short | |
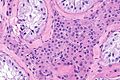
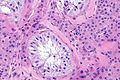
 Leydig cell hyperplasia. H&E stain. (WC) | |
|
| |
| LM | abundant Leydig cells interspersed between seminiferous tubules with only Sertoli cells, Leydig cells do not displace or compress the seminiferous tubules |
| LM DDx | Leydig cell tumour, testicular adrenal rest tumour |
| Site | testis, ovary |
|
| |
| Prevalence | rare |
| Radiology | hypoechoic lesions on ultrasound, often multiple |
| Prognosis | benign |
Leydig cell hyperplasia is an uncommon benign pathology of the testis.[1] It may be seen in the ovary.
General
- Benign.
- Uncommonly seen in isolation by pathology.
A longer list of causes:[2]
- Congenital (primary).
- Secondary causes:
- Germ cell loss/decrease:
- Cryptorchidism.
- Advanced age.
- Endocrine-related:
- Adrenal hyperplasia.
- Excess hCG - exogenous or tumour.
- Germ cell loss/decrease:
Other associations:[2]
- Klinefelter's syndrome.[3]
- Pernicious anemia.
- Alcoholism.
- Infection - syphilis, tuberculosis.
Gross
Features:
- Unremarkable gross appearance of parenchyma. (???)
- Normal or small testis. (???)
Note:
- Hypoechoic lesions on ultrasound - often multiple, small.[3]
Microscopic
Features:
- Abundant Leydig cells interspersed between seminiferous tubules with only Sertoli cells.
- Leydig cells do not displace or compress the seminiferous tubules.
Note:
- May form nodules up to 6 mm.[1]
DDx:
Images
LCH - very low mag. (WC)
LCH - very low mag. (WC)
LCH - low mag. (WC)
LCH - intermed. mag. (WC)
LCH - high mag. (WC)
LCH - high mag. (WC)





Sign out
Testicle and Cord, Right, Orchitectomy: - Leydig cell hyperplasia. - Atrophic testis. - NEGATIVE for germ cell neoplasia in situ (intratubular germ cell neoplasia). - NEGATIVE for malignancy. Comment: Immunostains confirm the morphologic impression. The Leydig cells are POSITIVE for inhibin, calretinin and melan A. The section is NEGATIVE for PLAP and has a benign pattern for D2-40.
See also
References
- ↑ 1.0 1.1 Carucci, LR.; Tirkes, AT.; Pretorius, ES.; Genega, EM.; Weinstein, SP. (Feb 2003). "Testicular Leydig's cell hyperplasia: MR imaging and sonographic findings.". AJR Am J Roentgenol 180 (2): 501-3. doi:10.2214/ajr.180.2.1800501. PMID 12540460.
- ↑ 2.0 2.1 Naughton, CK.; Nadler, RB.; Basler, JW.; Humphrey, PA. (Feb 1998). "Leydig cell hyperplasia.". Br J Urol 81 (2): 282-9. doi:10.1046/j.1464-410X.1998.00503.x. PMID 9488073.
- ↑ 3.0 3.1 Sterbis, J.; E-Nunu, T. (2015). "Leydig cell hyperplasia in the setting of Klinefelter syndrome.". BMJ Case Rep 2015. doi:10.1136/bcr-2015-209805. PMID 26209412.