Difference between revisions of "Small intestine"
| Line 210: | Line 210: | ||
==Meckel diverticulum== | ==Meckel diverticulum== | ||
{{Main|Meckel diverticulum}} | |||
==Ischemic enteritis== | ==Ischemic enteritis== | ||
Revision as of 20:38, 22 March 2016

The small intestine, also small bowel, is a relatively well-behaved piece of machinery from the perspective of pathology. It is uncommonly affected by malignancies, relative to its length when compared to the colon and rectum.
Normal small bowel
- AKA normal small intestine.
Anatomy
Consists of three segments:
- Duodenum - can be divided into four parts.
- Jejunum.
- Ileum.
The later two parts keep general surgeons awake at night (quite literally) 'cause they get obstructed and need urgent operations.
Length
- Normal length of small bowel = 3-8 metres.[1]
"Short":
- Less than 200 cm = short bowel syndrome.[2][3]
- Less than 100 cm usu. requires parenteral nutrition.[4]
Histology
The Gastrointestinal pathology article covers basic histology of the GI tract.
Immunohistochemistry
- Normal small intestine is CK20 +ve... while adenocarcinoma of the small bowel may be CK20 -ve.[5]
Sign out
Small Bowel, Biopsy: - Small bowel mucosa within normal limits.
Terminal Ileum, Biopsy: - Small bowel mucosa within normal limits.
Terminal Ileum, Biopsy: - Small bowel mucosa with morphologically benign lymphoid aggregates, negative for significant pathology.
Roux-en-Y gastric bypass
Small Bowel, Excision during Roux-en-Y Gastric Bypass: - Small bowel wall within normal limits.
Block letters
SMALL BOWEL, BIOPSY: - SMALL BOWEL MUCOSA WITHIN NORMAL LIMITS.
TERMINAL ILEUM, BIOPSY: - SMALL BOWEL MUCOSA WITHIN NORMAL LIMITS.
TERMINAL ILEUM, BIOPSY: - SMALL BOWEL MUCOSA WITH MORPHOLOGICAL BENIGN LYMPHOID AGGREGATES, NO SIGNIFICANT PATHOLOGY.
The segments
Duodenum
The duodenum is often biopsied by gastroenterologists.
Common reasons for biopsy:
- Suspected giardia.
- Suspected celiac sprue.
- Is this cancer?
- Looks normal... want to dot the i's and cross the t's.
Jejunum
- Uncommonly seen by pathologists.
- May be seen in the context of a resection done for a bowel obstruction.
Ileum
- This is seen occasionally -- often in the context of IBD and more specifically Crohn's disease.
- Crohn's disease andulcerative colitis are discussed in their respective articles.
Specific diagnoses
Ileitis
- Active ileitis and acute ileitis redirect here.
- This deals with nonspecific ileitis.
General
- Common.
Microscopic
Features:
- Intraepithelial neutrophils.
DDx:
- Crohn's disease.
- Infectious ileitis.
- Benign ileum - may have focal intra-epithelial lymphocytes associated with lamina propria lymphoid nodules.
Images

Ileitis - very low mag. (WC)
Ileitis - low mag. (WC)

Ileitis - intermed. mag. (WC)
Ileitis - high mag. (WC)




Small bowel obstruction
- Abbreviated SBO.
Small bowel neoplasms
- Adenocarcinoma - like colonic.
- Adenosquamous carcinoma.
- Neuroendocrine tumour.
- GIST.
- Schwannoma.
- Classically have a peripheral lymphoid cuff.[6]
Mechanical small bowel perforation
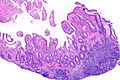
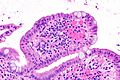
Ileal nodular lymphoid hyperplasia
- AKA nodular lymphoid hyperplasia of the terminal ileum.
General
- An uncommon diagnosis.
- May be associated with hypogammaglobulinemia.[7]
Gross
- Mucosal nodularity.
Microscopic
Features:
- Lymphoid nodules +/- germinal centre formation.
Note:
- Tingible body macrophages suggest an aggregate is benign.
DDx:
- MALT lymphoma.
- Mantle cell lymphoma.
- Other lymphomas.
IHC
- CD20 and CD3 - mixed population of lymphocytes.
- CD23 - follicular dendritic cells.
- Cyclin D1 -ve.
Note:
- IHC should be used if there is:
- Clinical suspicion.
- Histologic suspicion - either:
- Sheets of lymphocytes without apparent germinal centre formation in a larger area (~ 2 mm).
- Lymphoepithelial lesions.
Sign out
TERMINAL ILEUM, BIOPSY: - SMALL BOWEL MUCOSA WITH LYMPHOID NODULES WITH GERMINAL CENTRE FORMATION -- NO SIGNIFICANT PATHOLOGY. - NEGATIVE FOR ILEITIS.
TERMINAL ILEUM, BIOPSY: - SMALL BOWEL MUCOSA WITH LYMPHOID HYPERPLASIA -- NO SIGNIFICANT PATHOLOGY.
Micro
The sections show small bowel mucosa with lymphoid hyperplasia.
Immunostains for CD3 and CD20 show a mixed population of lymphocytes. A CD23 immunostain shows follicular dendritic cell networks. A cyclin D1 immunostain is negative.
Alternate
Immunostains for CD3 and CD20 show a mixed population of lymphocytes, with CD20 cells predominating. A cyclin D1 immunostain is negative. A CD23 immunostain shows follicular dendritic cell networks.
Multiple lymphomatous polyposis
- Abbreviated MLP.
- AKA lymphomatous polyposis.
General
- MLP is classically due to mantle cell lymphoma.[8]
- May be due to other lymphomas, e.g. follicular lymphoma.[9]
Microscopic
Features:
- Lymphoid nodules consisting of (small) atypical lymphocytes with an abnormal architecture.
IHC
See small cell lymphomas.
Small bowel diaphragm disease
- AKA diaphragm disease.
General
Microscopic
Features:[10]
- Focal submucosal fibrosis.
- +/-Distortion of adjacent muscularis propria.
- +/-Adjacent mucosal erosions/granulation tissue.
DDx:
- Cryptogenic multifocal ulcerous stenosing enteritis.[11] (???)
- Crohn's disease.
Meckel diverticulum
Ischemic enteritis
General
- Typically elderly and due to atherosclerosis.
- Rare.
- High mortality.[12]
- May occur together with ischemia of the colon, i.e. ischemic colitis, in which case it is known as ischemic enterocolitis.
Etiologies:
- Atherosclerosis.
- Vasculitis.
- Embolism.
- Thrombosis.
Microscopic
Features:
- See ischemic colitis.
DDx:
- Infection.
- Crohn's disease.
- Radiation changes.
- Drugs/toxins.
Weird stuff
Autoimmune enteropathy
- Abbreviated as AIE.
See also
References
- ↑ Nightingale, JM.. "Management of patients with a short bowel.". Nutrition 15 (7-8): 633-7. PMID 10422101.
- ↑ Donohoe, CL.; Reynolds, JV. (Oct 2010). "Short bowel syndrome.". Surgeon 8 (5): 270-9. doi:10.1016/j.surge.2010.06.004. PMID 20709285.
- ↑ Matarese, LE.; O'Keefe, SJ.; Kandil, HM.; Bond, G.; Costa, G.; Abu-Elmagd, K. (Oct 2005). "Short bowel syndrome: clinical guidelines for nutrition management.". Nutr Clin Pract 20 (5): 493-502. PMID 16207689.
- ↑ Sundaram, A.; Koutkia, P.; Apovian, CM. (Mar 2002). "Nutritional management of short bowel syndrome in adults.". J Clin Gastroenterol 34 (3): 207-20. PMID 11873098.
- ↑ Chen ZM, Wang HL (October 2004). "Alteration of cytokeratin 7 and cytokeratin 20 expression profile is uniquely associated with tumorigenesis of primary adenocarcinoma of the small intestine". Am. J. Surg. Pathol. 28 (10): 1352–9. PMID 15371952.
- ↑ Levy AD, Quiles AM, Miettinen M, Sobin LH (March 2005). "Gastrointestinal schwannomas: CT features with clinicopathologic correlation". AJR Am J Roentgenol 184 (3): 797–802. PMID 15728600. http://www.ajronline.org/cgi/content/full/184/3/797.
- ↑ Yamaue H, Tanimura H, Ishimoto K, Morikawa Y, Kakudo K (1996). "Nodular lymphoid hyperplasia of the terminal ileum: report of a case and the findings of an immunological analysis". Surg. Today 26 (6): 431-4. PMID 8782302.
- ↑ Ruskoné-Fourmestraux, A.; Audouin, J. (Feb 2010). "Primary gastrointestinal tract mantle cell lymphoma as multiple lymphomatous polyposis.". Best Pract Res Clin Gastroenterol 24 (1): 35-42. doi:10.1016/j.bpg.2009.12.001. PMID 20206107.
- ↑ URL: http://www.pathmax.com/gilymph.html. Accessed on: 1 April 2012.
- ↑ 10.0 10.1 McCune KH, Allen D, Cranley B (October 1992). "Small bowel diaphragm disease--strictures associated with non-steroidal anti-inflammatory drugs". Ulster Med J 61 (2): 182–4. PMC 2448949. PMID 1481311. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2448949/.
- ↑ Chung, SH.; Jo, Y.; Ryu, SR.; Ahn, SB.; Son, BK.; Kim, SH.; Park, YS.; Hong, YO. (Jun 2011). "Diaphragm disease compared with cryptogenic multifocal ulcerous stenosing enteritis.". World J Gastroenterol 17 (23): 2873-6. doi:10.3748/wjg.v17.i23.2873. PMID 21734797.
- ↑ Nakase, H. (Jul 2008). "[Ischemic enteritis].". Nihon Rinsho 66 (7): 1330-4. PMID 18616124.