Difference between revisions of "Oligodendroglioma"
Jump to navigation
Jump to search
Jensflorian (talk | contribs) (update) |
|||
| Line 33: | Line 33: | ||
==General== | ==General== | ||
*Do ''not'' arise from oligodendrocytes. | *Do ''not'' arise from oligodendrocytes, although tumor cells look very similiar.<ref>{{Cite journal | last1 = Hartmann | first1 = C. | last2 = von Deimling | first2 = A. | title = Molecular pathology of oligodendroglial tumors. | journal = Recent Results Cancer Res | volume = 171 | issue = | pages = 25-49 | month = | year = 2009 | doi = 10.1007/978-3-540-31206-2_2 | PMID = 19322536 }}</ref> | ||
**Arise from ''glial precursor cells''. | **Arise from ''glial precursor cells''. | ||
| Line 39: | Line 39: | ||
*WHO grade II: 10-15 years. | *WHO grade II: 10-15 years. | ||
*WHO grade III: 3-5 years. | *WHO grade III: 3-5 years. | ||
Oligodendrogliomas account for approx 5% of all [[glioma]]s. | |||
* Numbers may be higher when stringent classifiation criteria are not applied. | |||
* Peak incidence: 40-45 years. | |||
* First description of the tumor in 1926. | |||
*WHO Grade II: ICD-O: 9450/3. | |||
*WHO Grade III: ICD-O: 9451/3. | |||
==Gross/radiologic== | ==Gross/radiologic== | ||
Location: | Location: | ||
*Cerebral hemispheres - most often frontal lobe, followed by parietal and temporal lobes.<ref name=Ref_PSNP94>{{Ref PSNP|94}}</ref> | *Cerebral hemispheres - most often (50-60%) frontal lobe, followed by parietal and temporal lobes.<ref name=Ref_PSNP94>{{Ref PSNP|94}}</ref> | ||
*Posterior fossa (rare). | *Posterior fossa (rare). | ||
*Intramedullary spinal cord (very rare). | *Intramedullary spinal cord (very rare). | ||
| Line 51: | Line 59: | ||
*Nonenhancing or enhancing. | *Nonenhancing or enhancing. | ||
*Occasionally well-circumscribed. | *Occasionally well-circumscribed. | ||
Clinical symptoms: | |||
*Seizures. | |||
*Intracranial pressure. | |||
*Focal neurologic decifits. | |||
*Cognitive changes. | |||
==Microscopic== | ==Microscopic== | ||
Features: | Features: | ||
*Diffusely growing tumor. | |||
*Highly cellular lesion composed of: | *Highly cellular lesion composed of: | ||
**Cells resembling ''fried eggs'' (oligodendrocytes) with: | **Cells resembling ''fried eggs'' (oligodendrocytes) with: | ||
| Line 64: | Line 79: | ||
***Abundant, delicate appearing; may vaguely resemble a paraganglioma at low power. | ***Abundant, delicate appearing; may vaguely resemble a paraganglioma at low power. | ||
*Calcifications - important feature.<ref>URL: [http://www.emedicine.com/radio/topic481.htm http://www.emedicine.com/radio/topic481.htm].</ref> | *Calcifications - important feature.<ref>URL: [http://www.emedicine.com/radio/topic481.htm http://www.emedicine.com/radio/topic481.htm].</ref> | ||
*Perifocal edema uncommon. | |||
*Few tumors may exhibit [[eosinophilic granular bodies]]. | |||
*Some tumors may show a [[Spongioblastoma]]-like growth pattern. | |||
Anaplastic (grade III) criteria:<ref>{{Cite journal | last1 = Giannini | first1 = C. | last2 = Scheithauer | first2 = BW. | last3 = Weaver | first3 = AL. | last4 = Burger | first4 = PC. | last5 = Kros | first5 = JM. | last6 = Mork | first6 = S. | last7 = Graeber | first7 = MB. | last8 = Bauserman | first8 = S. | last9 = Buckner | first9 = JC. | title = Oligodendrogliomas: reproducibility and prognostic value of histologic diagnosis and grading. | journal = J Neuropathol Exp Neurol | volume = 60 | issue = 3 | pages = 248-62 | month = Mar | year = 2001 | doi = | PMID = 11245209 }}</ref> | |||
*"Significant" or "brisk" mitotic activity. | |||
**That means for most neuropathologists >= 6 mitoses per 10 HPF. | |||
*Microvacular proliferation. | |||
*Necrosis. | |||
Note: | Note: | ||
*Tumour cells may be plasmacytoid, i.e. have a [[plasma cell]]-like appearance.<ref name=pmid17284109>{{Cite journal | last1 = Aldape | first1 = K. | last2 = Burger | first2 = PC. | last3 = Perry | first3 = A. | title = Clinicopathologic aspects of 1p/19q loss and the diagnosis of oligodendroglioma. | journal = Arch Pathol Lab Med | volume = 131 | issue = 2 | pages = 242-51 | month = Feb | year = 2007 | doi = 10.1043/1543-2165(2007)131[242:CAOQLA]2.0.CO;2 | PMID = 17284109 | URL = http://www.archivesofpathology.org/doi/full/10.1043/1543-2165(2007)131%5B242:CAOQLA%5D2.0.CO;2 }}</ref> | * Tumour cells may be plasmacytoid, i.e. have a [[plasma cell]]-like appearance.<ref name=pmid17284109>{{Cite journal | last1 = Aldape | first1 = K. | last2 = Burger | first2 = PC. | last3 = Perry | first3 = A. | title = Clinicopathologic aspects of 1p/19q loss and the diagnosis of oligodendroglioma. | journal = Arch Pathol Lab Med | volume = 131 | issue = 2 | pages = 242-51 | month = Feb | year = 2007 | doi = 10.1043/1543-2165(2007)131[242:CAOQLA]2.0.CO;2 | PMID = 17284109 | URL = http://www.archivesofpathology.org/doi/full/10.1043/1543-2165(2007)131%5B242:CAOQLA%5D2.0.CO;2 }}</ref> | ||
**Also called minigemistocytes. | |||
**The are usually strong GFAP+ve. | |||
DDx: | DDx: | ||
*[[Neurocytoma]] also have perinuclear clearing and well-defined cellular borders. | *[[Neurocytoma]] also have perinuclear clearing and well-defined cellular borders. | ||
**Pineocytomatous/neurocytic rosettes = (irregular) rosette with a large meshwork of fibers (neuropil) at the centre. | **Pineocytomatous/neurocytic rosettes = (irregular) rosette with a large meshwork of fibers (neuropil) at the centre. | ||
*Clear cell [[ependymoma]]. | |||
*[[Dysembryoplastic neuroepithelial tumor]]. | |||
*Oligodendroglial-like cells in [[Pilocytic astrocytoma]]. | |||
*Clear cell [[meningioma]]. | |||
*Demyelinisation. | |||
Notes: | Notes: | ||
| Line 83: | Line 115: | ||
Image:Oligodendroglioma1_high_mag.jpg | Oligodendroglioma high mag. (WC) | Image:Oligodendroglioma1_high_mag.jpg | Oligodendroglioma high mag. (WC) | ||
Image:Oligodendroglioma1_low_mag.jpg | Oligodendroglioma low mag. (WC) | Image:Oligodendroglioma1_low_mag.jpg | Oligodendroglioma low mag. (WC) | ||
File:Oligodendroglioma_discrete_invasion_HE.jpg | Discrete invasion in a oligodendroglioma. (WC/jensflorian). | |||
</gallery> | </gallery> | ||
www: | www: | ||
*[http://path.upmc.edu/cases/case713.html Oligodendroglioma - several images (upmc.edu)]. | *[http://path.upmc.edu/cases/case713.html Oligodendroglioma - several images (upmc.edu)]. | ||
| Line 105: | Line 139: | ||
**Some subtypes +ve - should not be used to distinguish.<ref name=Ref_PSNP>{{Ref PSNP|98}}</ref> | **Some subtypes +ve - should not be used to distinguish.<ref name=Ref_PSNP>{{Ref PSNP|98}}</ref> | ||
*EMA +ve. | *EMA +ve. | ||
*IDH-1 | *IDH-1 (R132H) +ve (approx 85%). | ||
**18% +ve in one series of children,<ref name=pmid24805856>{{Cite journal | last1 = Rodriguez | first1 = FJ. | last2 = Tihan | first2 = T. | last3 = Lin | first3 = D. | last4 = McDonald | first4 = W. | last5 = Nigro | first5 = J. | last6 = Feuerstein | first6 = B. | last7 = Jackson | first7 = S. | last8 = Cohen | first8 = K. | last9 = Burger | first9 = PC. | title = Clinicopathologic features of pediatric oligodendrogliomas: a series of 50 patients. | journal = Am J Surg Pathol | volume = 38 | issue = 8 | pages = 1058-70 | month = Aug | year = 2014 | doi = 10.1097/PAS.0000000000000221 | PMID = 24805856 }}</ref> 23% +ve in another series.<ref name=pmid23361281>{{Cite journal | last1 = Sipayya | first1 = V. | last2 = Sharma | first2 = I. | last3 = Sharma | first3 = KC. | last4 = Singh | first4 = A. | title = Immunohistochemical expression of IDH1 in gliomas: a tissue microarray-based approach. | journal = J Cancer Res Ther | volume = 8 | issue = 4 | pages = 598-601 | month = | year = | doi = 10.4103/0973-1482.106567 | PMID = 23361281 }}</ref> | **18% +ve in one series of children,<ref name=pmid24805856>{{Cite journal | last1 = Rodriguez | first1 = FJ. | last2 = Tihan | first2 = T. | last3 = Lin | first3 = D. | last4 = McDonald | first4 = W. | last5 = Nigro | first5 = J. | last6 = Feuerstein | first6 = B. | last7 = Jackson | first7 = S. | last8 = Cohen | first8 = K. | last9 = Burger | first9 = PC. | title = Clinicopathologic features of pediatric oligodendrogliomas: a series of 50 patients. | journal = Am J Surg Pathol | volume = 38 | issue = 8 | pages = 1058-70 | month = Aug | year = 2014 | doi = 10.1097/PAS.0000000000000221 | PMID = 24805856 }}</ref> 23% +ve in another series.<ref name=pmid23361281>{{Cite journal | last1 = Sipayya | first1 = V. | last2 = Sharma | first2 = I. | last3 = Sharma | first3 = KC. | last4 = Singh | first4 = A. | title = Immunohistochemical expression of IDH1 in gliomas: a tissue microarray-based approach. | journal = J Cancer Res Ther | volume = 8 | issue = 4 | pages = 598-601 | month = | year = | doi = 10.4103/0973-1482.106567 | PMID = 23361281 }}</ref> | ||
*ATRX +ve. | |||
**Useful for differentiating ''astrocytoma'' vs. ''oligodendroglioma''.<ref>{{Cite journal | last1 = Reuss | first1 = DE. | last2 = Sahm | first2 = F. | last3 = Schrimpf | first3 = D. | last4 = Wiestler | first4 = B. | last5 = Capper | first5 = D. | last6 = Koelsche | first6 = C. | last7 = Schweizer | first7 = L. | last8 = Korshunov | first8 = A. | last9 = Jones | first9 = DT. | title = ATRX and IDH1-R132H immunohistochemistry with subsequent copy number analysis and IDH sequencing as a basis for an "integrated" diagnostic approach for adult astrocytoma, oligodendroglioma and glioblastoma. | journal = Acta Neuropathol | volume = 129 | issue = 1 | pages = 133-46 | month = Jan | year = 2015 | doi = 10.1007/s00401-014-1370-3 | PMID = 25427834 }}</ref> | |||
*p53 -ve. | *p53 -ve. | ||
* | *Ki-67 (usu. >5% in grade II). | ||
* | *May have neuronal "islands" (Synapto +ve, NeuN +ve). | ||
==Molecular pathology== | ==Molecular pathology== | ||
Combined losses of 1p and 19q both helps with diagnosis and is prognostic and therapeutic relevant:<ref name=pmid18565359>{{cite journal |author=Fontaine D, Vandenbos F, Lebrun C, Paquis V, Frenay M |title=[Diagnostic and prognostic values of 1p and 19q deletions in adult gliomas: critical review of the literature and implications in daily clinical practice] |language=French |journal=Rev. Neurol. (Paris) |volume=164 |issue=6-7 |pages=595–604 |year=2008 |pmid=18565359 |doi=10.1016/j.neurol.2008.04.002 |url=}}</ref><ref>{{Cite journal | last1 = Wiestler | first1 = B. | last2 = Capper | first2 = D. | last3 = Hovestadt | first3 = V. | last4 = Sill | first4 = M. | last5 = Jones | first5 = DT. | last6 = Hartmann | first6 = C. | last7 = Felsberg | first7 = J. | last8 = Platten | first8 = M. | last9 = Feiden | first9 = W. | title = Assessing CpG island methylator phenotype, 1p/19q codeletion, and MGMT promoter methylation from epigenome-wide data in the biomarker cohort of the NOA-04 trial. | journal = Neuro Oncol | volume = 16 | issue = 12 | pages = 1630-8 | month = Dec | year = 2014 | doi = 10.1093/neuonc/nou138 | PMID = 25028501 }}</ref><ref>{{Cite journal | last1 = Cairncross | first1 = G. | last2 = Wang | first2 = M. | last3 = Shaw | first3 = E. | last4 = Jenkins | first4 = R. | last5 = Brachman | first5 = D. | last6 = Buckner | first6 = J. | last7 = Fink | first7 = K. | last8 = Souhami | first8 = L. | last9 = Laperriere | first9 = N. | title = Phase III trial of chemoradiotherapy for anaplastic oligodendroglioma: long-term results of RTOG 9402. | journal = J Clin Oncol | volume = 31 | issue = 3 | pages = 337-43 | month = Jan | year = 2013 | doi = 10.1200/JCO.2012.43.2674 | PMID = 23071247 }}</ref> | |||
*Greater chemosensitivity | *Greater chemosensitivity | ||
*Better prognosis. | *Better prognosis. | ||
Note: | |||
*Consider underdiagnosed Glioblastoma, when tumor is IDH1/2 wildtype and has no LOH 1p/19q and/or ATRX loss. | |||
**It is very likely in the future, that non-codeleted tumors are no longer classified as oligodendrogliomas on molecular basis. | |||
==See also== | ==See also== | ||
Revision as of 10:08, 15 June 2015
| Oligodendroglioma | |
|---|---|
| Diagnosis in short | |
 Oligodendroglioma. H&E stain. | |
|
| |
| LM | highly cellular lesion composed of cells resembling fried eggs (oligodendrocytes) with a round nucleus (important), distinct cell borders, +/-clear cytoplasm - useful feature (if present), acutely branched capillary sized vessels ("chicken-wire" like appearance), calcifications |
| LM DDx | neurocytoma, clear cell variant of ependymoma, seminoma / dysgerminoma / germinoma |
| Molecular | +/-loss of 1p and 19q (common) |
| Site | neuropathology tumours - cerebral hemispheres, posterior fossa (rare), spinal cord (very rare) |
|
| |
| Radiology | intra-axial mass, +/-calcifications (best seen on CT), nonenhancing or enhancing |
| Prognosis | moderate - dependent on grade |
Oligodendroglioma is CNS tumour that is typically in the cerebral hemispheres.
General
- Do not arise from oligodendrocytes, although tumor cells look very similiar.[1]
- Arise from glial precursor cells.
Prognosis by flavours (average survival):[2]
- WHO grade II: 10-15 years.
- WHO grade III: 3-5 years.
Oligodendrogliomas account for approx 5% of all gliomas.
- Numbers may be higher when stringent classifiation criteria are not applied.
- Peak incidence: 40-45 years.
- First description of the tumor in 1926.
- WHO Grade II: ICD-O: 9450/3.
- WHO Grade III: ICD-O: 9451/3.
Gross/radiologic
Location:
- Cerebral hemispheres - most often (50-60%) frontal lobe, followed by parietal and temporal lobes.[3]
- Posterior fossa (rare).
- Intramedullary spinal cord (very rare).
Radiologic features:[3]
- Intra-axial mass.
- +/-Calcifications (best seen on CT).
- Nonenhancing or enhancing.
- Occasionally well-circumscribed.
Clinical symptoms:
- Seizures.
- Intracranial pressure.
- Focal neurologic decifits.
- Cognitive changes.
Microscopic
Features:
- Diffusely growing tumor.
- Highly cellular lesion composed of:
- Cells resembling fried eggs (oligodendrocytes) with:
- Round nucleus - key feature.
- Distinct cell borders.
- Moderate-to-marked nuclear atypia.
- Clear cytoplasm - useful feature (if present).
- Some oligodendrogliomas have eosinophilic cytoplasm with focal perinuclear clearing.
- Acutely branched capillary sized vessels - "chicken-wire" like appearance.
- Abundant, delicate appearing; may vaguely resemble a paraganglioma at low power.
- Cells resembling fried eggs (oligodendrocytes) with:
- Calcifications - important feature.[4]
- Perifocal edema uncommon.
- Few tumors may exhibit eosinophilic granular bodies.
- Some tumors may show a Spongioblastoma-like growth pattern.
Anaplastic (grade III) criteria:[5]
- "Significant" or "brisk" mitotic activity.
- That means for most neuropathologists >= 6 mitoses per 10 HPF.
- Microvacular proliferation.
- Necrosis.
Note:
- Tumour cells may be plasmacytoid, i.e. have a plasma cell-like appearance.[6]
- Also called minigemistocytes.
- The are usually strong GFAP+ve.
DDx:
- Neurocytoma also have perinuclear clearing and well-defined cellular borders.
- Pineocytomatous/neurocytic rosettes = (irregular) rosette with a large meshwork of fibers (neuropil) at the centre.
- Clear cell ependymoma.
- Dysembryoplastic neuroepithelial tumor.
- Oligodendroglial-like cells in Pilocytic astrocytoma.
- Clear cell meningioma.
- Demyelinisation.
Notes:
- Few neural tumours have round nuclei - DDx:
- Oligodendroglioma.
- Lymphoma.
- Clear cell variant of ependymoma.
- Germ cell tumour (germinoma/dysgerminoma/seminoma).
Images
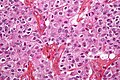
Oligodendroglioma high mag. (WC)
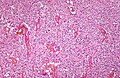
Oligodendroglioma low mag. (WC)

Discrete invasion in a oligodendroglioma. (WC/jensflorian).


www:
- Oligodendroglioma - several images (upmc.edu).
- Oligodendroglioma with plasmacytoid cells (frontalcortex.com).
Histologic grading
Come in two flavours:
- WHO grade II.
- This is most oligodendrogliomas.
- WHO grade III.
IHC
Features:
- MAP-2 +ve.[7]
- GFAP +ve (variable).
- Some subtypes +ve - should not be used to distinguish.[8]
- EMA +ve.
- IDH-1 (R132H) +ve (approx 85%).
- ATRX +ve.
- Useful for differentiating astrocytoma vs. oligodendroglioma.[11]
- p53 -ve.
- Ki-67 (usu. >5% in grade II).
- May have neuronal "islands" (Synapto +ve, NeuN +ve).
Molecular pathology
Combined losses of 1p and 19q both helps with diagnosis and is prognostic and therapeutic relevant:[12][13][14]
- Greater chemosensitivity
- Better prognosis.
Note:
- Consider underdiagnosed Glioblastoma, when tumor is IDH1/2 wildtype and has no LOH 1p/19q and/or ATRX loss.
- It is very likely in the future, that non-codeleted tumors are no longer classified as oligodendrogliomas on molecular basis.
See also
References
- ↑ Hartmann, C.; von Deimling, A. (2009). "Molecular pathology of oligodendroglial tumors.". Recent Results Cancer Res 171: 25-49. doi:10.1007/978-3-540-31206-2_2. PMID 19322536.
- ↑ 2.0 2.1 Perry, Arie; Brat, Daniel J. (2010). Practical Surgical Neuropathology: A Diagnostic Approach: A Volume in the Pattern Recognition series (1st ed.). Churchill Livingstone. pp. 98. ISBN 978-0443069826.
- ↑ 3.0 3.1 Perry, Arie; Brat, Daniel J. (2010). Practical Surgical Neuropathology: A Diagnostic Approach: A Volume in the Pattern Recognition series (1st ed.). Churchill Livingstone. pp. 94. ISBN 978-0443069826.
- ↑ URL: http://www.emedicine.com/radio/topic481.htm.
- ↑ Giannini, C.; Scheithauer, BW.; Weaver, AL.; Burger, PC.; Kros, JM.; Mork, S.; Graeber, MB.; Bauserman, S. et al. (Mar 2001). "Oligodendrogliomas: reproducibility and prognostic value of histologic diagnosis and grading.". J Neuropathol Exp Neurol 60 (3): 248-62. PMID 11245209.
- ↑ Aldape, K.; Burger, PC.; Perry, A. (Feb 2007). "Clinicopathologic aspects of 1p/19q loss and the diagnosis of oligodendroglioma.". Arch Pathol Lab Med 131 (2): 242-51. doi:10.1043/1543-2165(2007)131[242:CAOQLA]2.0.CO;2. PMID 17284109.
- ↑ Suzuki SO, Kitai R, Llena J, Lee SC, Goldman JE, Shafit-Zagardo B (May 2002). "MAP-2e, a novel MAP-2 isoform, is expressed in gliomas and delineates tumor architecture and patterns of infiltration". J. Neuropathol. Exp. Neurol. 61 (5): 403–12. PMID 12025943.
- ↑ Perry, Arie; Brat, Daniel J. (2010). Practical Surgical Neuropathology: A Diagnostic Approach: A Volume in the Pattern Recognition series (1st ed.). Churchill Livingstone. pp. 98. ISBN 978-0443069826.
- ↑ Rodriguez, FJ.; Tihan, T.; Lin, D.; McDonald, W.; Nigro, J.; Feuerstein, B.; Jackson, S.; Cohen, K. et al. (Aug 2014). "Clinicopathologic features of pediatric oligodendrogliomas: a series of 50 patients.". Am J Surg Pathol 38 (8): 1058-70. doi:10.1097/PAS.0000000000000221. PMID 24805856.
- ↑ Sipayya, V.; Sharma, I.; Sharma, KC.; Singh, A.. "Immunohistochemical expression of IDH1 in gliomas: a tissue microarray-based approach.". J Cancer Res Ther 8 (4): 598-601. doi:10.4103/0973-1482.106567. PMID 23361281.
- ↑ Reuss, DE.; Sahm, F.; Schrimpf, D.; Wiestler, B.; Capper, D.; Koelsche, C.; Schweizer, L.; Korshunov, A. et al. (Jan 2015). "ATRX and IDH1-R132H immunohistochemistry with subsequent copy number analysis and IDH sequencing as a basis for an "integrated" diagnostic approach for adult astrocytoma, oligodendroglioma and glioblastoma.". Acta Neuropathol 129 (1): 133-46. doi:10.1007/s00401-014-1370-3. PMID 25427834.
- ↑ Fontaine D, Vandenbos F, Lebrun C, Paquis V, Frenay M (2008). "[Diagnostic and prognostic values of 1p and 19q deletions in adult gliomas: critical review of the literature and implications in daily clinical practice]" (in French). Rev. Neurol. (Paris) 164 (6-7): 595–604. doi:10.1016/j.neurol.2008.04.002. PMID 18565359.
- ↑ Wiestler, B.; Capper, D.; Hovestadt, V.; Sill, M.; Jones, DT.; Hartmann, C.; Felsberg, J.; Platten, M. et al. (Dec 2014). "Assessing CpG island methylator phenotype, 1p/19q codeletion, and MGMT promoter methylation from epigenome-wide data in the biomarker cohort of the NOA-04 trial.". Neuro Oncol 16 (12): 1630-8. doi:10.1093/neuonc/nou138. PMID 25028501.
- ↑ Cairncross, G.; Wang, M.; Shaw, E.; Jenkins, R.; Brachman, D.; Buckner, J.; Fink, K.; Souhami, L. et al. (Jan 2013). "Phase III trial of chemoradiotherapy for anaplastic oligodendroglioma: long-term results of RTOG 9402.". J Clin Oncol 31 (3): 337-43. doi:10.1200/JCO.2012.43.2674. PMID 23071247.