Difference between revisions of "Apocrine carcinoma of the breast"
Jump to navigation
Jump to search
(→IHC) |
|||
| Line 1: | Line 1: | ||
{{ Infobox diagnosis | {{ Infobox diagnosis | ||
| Name = {{PAGENAME}} | | Name = {{PAGENAME}} | ||
| Image = | | Image = Breast ApocrineCarcinoma MP2 CTR.jpg | ||
| Width = | | Width = | ||
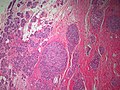
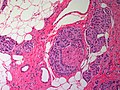
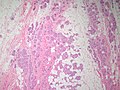
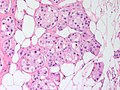
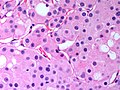
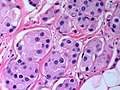
| Caption = | | Caption = Apocrine carcinoma of the breast. [[H&E stain]]. | ||
| Synonyms = | | Synonyms = | ||
| Micro = apocrine morphology (cells with prominent [[nucleoli]] - may be multiple, abundant granular eosinophilic cytoplasm) - must be >=90% of tumour, loss of basal cells | | Micro = apocrine morphology (cells with prominent [[nucleoli]] - may be multiple, abundant granular eosinophilic cytoplasm) - must be >=90% of tumour, loss of basal cells | ||
| Line 25: | Line 25: | ||
| Rads = | | Rads = | ||
| Endoscopy = | | Endoscopy = | ||
| Prognosis = | | Prognosis = poor, worse the ductal carcinoma | ||
| Other = | | Other = | ||
| ClinDDx = | | ClinDDx = other breast masses | ||
| Tx = | | Tx = excision | ||
}} | }} | ||
'''Apocrine carcinoma of the breast''' is a rare form of [[invasive breast cancer]]. | '''Apocrine carcinoma of the breast''' is a rare form of [[invasive breast cancer]]. | ||
| Line 34: | Line 34: | ||
==General== | ==General== | ||
*Need >=90% apocrine morphology.<ref name=Ref_BP217>{{Ref BP|217}}</ref> | *Need >=90% apocrine morphology.<ref name=Ref_BP217>{{Ref BP|217}}</ref> | ||
*Worse prognosis that [[invasive ductal carcinoma of the breast]] in a large series.<ref name=pmid23245877>{{Cite journal | last1 = Dellapasqua | first1 = S. | last2 = Maisonneuve | first2 = P. | last3 = Viale | first3 = G. | last4 = Pruneri | first4 = G. | last5 = Mazzarol | first5 = G. | last6 = Ghisini | first6 = R. | last7 = Mazza | first7 = M. | last8 = Iorfida | first8 = M. | last9 = Rotmensz | first9 = N. | title = Immunohistochemically defined subtypes and outcome of apocrine breast cancer. | journal = Clin Breast Cancer | volume = 13 | issue = 2 | pages = 95-102 | month = Apr | year = 2013 | doi = 10.1016/j.clbc.2012.11.004 | PMID = 23245877 }}</ref> | |||
==Microscopic== | ==Microscopic== | ||
| Line 46: | Line 47: | ||
*Cutaneous Apocrine Carcinoma | *Cutaneous Apocrine Carcinoma | ||
***A possible cutaneous apocrine carcinoma in a patient with a history of mammary apocrine carcinoma is problematic but fortunately a relatively infrequent conundrum. | ***A possible cutaneous apocrine carcinoma in a patient with a history of mammary apocrine carcinoma is problematic but fortunately a relatively infrequent conundrum. | ||
*Apocrine-like carcinoma - immunoprolife doesn't fit for invasive AC (ER +ve, PR +ve, AR-ve).<ref name=pmid23245877/> | |||
===Images=== | ===Images=== | ||
| Line 66: | Line 68: | ||
*ER -ve. | *ER -ve. | ||
*PR -ve. | *PR -ve. | ||
*often | *often HER2 +ve but can be HER2 -ve<ref name=pmid19898421>{{Cite journal | last1 = Niemeier | first1 = LA. | last2 = Dabbs | first2 = DJ. | last3 = Beriwal | first3 = S. | last4 = Striebel | first4 = JM. | last5 = Bhargava | first5 = R. | title = Androgen receptor in breast cancer: expression in estrogen receptor-positive tumors and in estrogen receptor-negative tumors with apocrine differentiation. | journal = Mod Pathol | volume = 23 | issue = 2 | pages = 205-12 | month = Feb | year = 2010 | doi = 10.1038/modpathol.2009.159 | PMID = 19898421 }}</ref> | ||
Notes | Notes | ||
Revision as of 21:06, 1 April 2015
| Apocrine carcinoma of the breast | |
|---|---|
| Diagnosis in short | |
 Apocrine carcinoma of the breast. H&E stain. | |
|
| |
| LM | apocrine morphology (cells with prominent nucleoli - may be multiple, abundant granular eosinophilic cytoplasm) - must be >=90% of tumour, loss of basal cells |
| LM DDx | glycogen-rich clear cell carcinoma of the breast |
| IHC | AR +ve, GCDFP-15 +ve, ER -ve, PR -ve |
| Site | breast - see invasive breast cancer |
|
| |
| Prevalence | uncommon |
| Prognosis | poor, worse the ductal carcinoma |
| Clin. DDx | other breast masses |
| Treatment | excision |
Apocrine carcinoma of the breast is a rare form of invasive breast cancer.
General
- Need >=90% apocrine morphology.[1]
- Worse prognosis that invasive ductal carcinoma of the breast in a large series.[2]
Microscopic
Features:[1]
- Prominent nucleoli.
- Often multiple.[3]
- Abundant granular eosinophilic cytoplasm.
- Architecture like invasive ductal carcinomas no special type.
DDx:
- Glycogen-rich clear cell carcinoma of the breast.
- Cutaneous Apocrine Carcinoma
- A possible cutaneous apocrine carcinoma in a patient with a history of mammary apocrine carcinoma is problematic but fortunately a relatively infrequent conundrum.
- Apocrine-like carcinoma - immunoprolife doesn't fit for invasive AC (ER +ve, PR +ve, AR-ve).[2]
Images
www:
Breast - Apocrine Carcinoma - Low power (SKB)
Breast - Apocrine Carcinoma - Perineural invasion - High power (SKB)
Breast - Apocrine Carcinoma - Low power (SKB)
Breast - Apocrine Carcinoma - Medium power (SKB)
Breast - Apocrine Carcinoma - High power (SKB)
Breast - Apocrine Carcinoma - High power (SKB)





IHC
Smaller tumours classically:[4]
- AR +ve.
- GCDFP-15 +ve.
Usually:[1]
- ER -ve.
- PR -ve.
- often HER2 +ve but can be HER2 -ve[5]
Notes
- Salivary gland carcinoma and cutaneous adnexal tumors can show a similar IHC profile.
- Apocrine carcioma can be a non-basal type 'triple negative carcinoma' [6].
- May show different behaviour to other types of triple negative carcinoma
- May respond to treatments targeting the androgen receptor[7]
- Be careful when reading the literature in this area - is the author discussing 'molecular apocrine' (ER -ve, AR +ve) or 'morphologic apocrine' carcinoma.
- Many ductal carcinomas, NOS will show AR positivity but are often ER +ve.
See also
References
- ↑ 1.0 1.1 1.2 O'Malley, Frances P.; Pinder, Sarah E. (2006). Breast Pathology: A Volume in Foundations in Diagnostic Pathology series (1st ed.). Churchill Livingstone. pp. 217. ISBN 978-0443066801.
- ↑ 2.0 2.1 Dellapasqua, S.; Maisonneuve, P.; Viale, G.; Pruneri, G.; Mazzarol, G.; Ghisini, R.; Mazza, M.; Iorfida, M. et al. (Apr 2013). "Immunohistochemically defined subtypes and outcome of apocrine breast cancer.". Clin Breast Cancer 13 (2): 95-102. doi:10.1016/j.clbc.2012.11.004. PMID 23245877.
- ↑ O'Malley, FP.; Bane, A. (Jan 2008). "An update on apocrine lesions of the breast.". Histopathology 52 (1): 3-10. doi:10.1111/j.1365-2559.2007.02888.x. PMID 18171412.
- ↑ Honma, N.; Takubo, K.; Akiyama, F.; Sawabe, M.; Arai, T.; Younes, M.; Kasumi, F.; Sakamoto, G. (Aug 2005). "Expression of GCDFP-15 and AR decreases in larger or node-positive apocrine carcinomas of the breast.". Histopathology 47 (2): 195-201. doi:10.1111/j.1365-2559.2005.02181.x. PMID 16045781.
- ↑ Niemeier, LA.; Dabbs, DJ.; Beriwal, S.; Striebel, JM.; Bhargava, R. (Feb 2010). "Androgen receptor in breast cancer: expression in estrogen receptor-positive tumors and in estrogen receptor-negative tumors with apocrine differentiation.". Mod Pathol 23 (2): 205-12. doi:10.1038/modpathol.2009.159. PMID 19898421.
- ↑ Tsutsumi, Y. (May 2012). "Apocrine carcinoma as triple-negative breast cancer: novel definition of apocrine-type carcinoma as estrogen/progesterone receptor-negative and androgen receptor-positive invasive ductal carcinoma.". Jpn J Clin Oncol 42 (5): 375-86. doi:10.1093/jjco/hys034. PMID 22450930.
- ↑ Safarpour, D.; Tavassoli, FA. (Oct 2014). "A Targetable Androgen Receptor-Positive Breast Cancer Subtype Hidden Among the Triple-Negative Cancers.". Arch Pathol Lab Med. doi:10.5858/arpa.2014-0122-RA. PMID 25310144.