Difference between revisions of "Low-grade squamous intraepithelial lesion"
Jump to navigation
Jump to search
(+ihc) |
|||
| Line 76: | Line 76: | ||
*[http://www.flickr.com/photos/jian-hua_qiao_md/3987000055/ CIN 1 (flickr.com/Qiao)]. | *[http://www.flickr.com/photos/jian-hua_qiao_md/3987000055/ CIN 1 (flickr.com/Qiao)]. | ||
*[http://www.eurocytology.eu/static/eurocytology/eng/cervical/mod6img1a.html CIN 1 (eurocytology.eu)]. | *[http://www.eurocytology.eu/static/eurocytology/eng/cervical/mod6img1a.html CIN 1 (eurocytology.eu)]. | ||
==IHC== | |||
Features:<ref name=pmid22162342>{{Cite journal | last1 = Singh | first1 = M. | last2 = Mockler | first2 = D. | last3 = Akalin | first3 = A. | last4 = Burke | first4 = S. | last5 = Shroyer | first5 = A. | last6 = Shroyer | first6 = KR. | title = Immunocytochemical colocalization of P16(INK4a) and Ki-67 predicts CIN2/3 and AIS/adenocarcinoma. | journal = Cancer Cytopathol | volume = 120 | issue = 1 | pages = 26-34 | month = Feb | year = 2012 | doi = 10.1002/cncy.20188 | PMID = 22162342 }}</ref> | |||
*p16. | |||
**Diffuse strong staining involving at least all of the basal aspect of the epithelium = CIN II or CIN III. | |||
**Patchy, weak positive staining = CIN I or squamous metaplasia. | |||
*Ki-67. | |||
**Several positive cells above basal layer suggests CIN II or CIN III. | |||
Notes: | |||
*Both p16 and Ki-67 are usually negative in CIN I -- 75% of cases.<ref name=pmid22104735>{{Cite journal | last1 = Jackson | first1 = JA. | last2 = Kapur | first2 = U. | last3 = Erşahin | first3 = Ç. | title = Utility of p16, Ki-67, and HPV test in diagnosis of cervical intraepithelial neoplasia and atrophy in women older than 50 years with 3- to 7-year follow-up. | journal = Int J Surg Pathol | volume = 20 | issue = 2 | pages = 146-53 | month = Apr | year = 2012 | doi = 10.1177/1066896911427703 | PMID = 22104735 }}</ref> | |||
**CIN I with p16 staining appears to have a higher risk of progression the p16 negative CIN I.<ref name=pmid19683687>{{Cite journal | last1 = del Pino | first1 = M. | last2 = Garcia | first2 = S. | last3 = Fusté | first3 = V. | last4 = Alonso | first4 = I. | last5 = Fusté | first5 = P. | last6 = Torné | first6 = A. | last7 = Ordi | first7 = J. | title = Value of p16(INK4a) as a marker of progression/regression in cervical intraepithelial neoplasia grade 1. | journal = Am J Obstet Gynecol | volume = 201 | issue = 5 | pages = 488.e1-7 | month = Nov | year = 2009 | doi = 10.1016/j.ajog.2009.05.046 | PMID = 19683687 }}</ref> | |||
==See also== | ==See also== | ||
Revision as of 19:51, 30 January 2014
Low-grade squamous intraepithelial lesion, abbreviated LSIL, is a pre-cancerous lesions of the uterine cervix.
Increasingly, the term is being applied to other anatomical sites, e.g. vagina.
It is in the larger category of squamous intraepithelial lesion, abbreviated SIL.
General
- Precursor lesion of cervical squamous cell carcinoma.
- Usually associated with human papilloma virus.
SIL is divided into grades:
- Low-grade.
- High-grade.
The new and old terminology
| SIL (current terminology) | LSIL | HSIL |
|---|---|---|
| Recent terminology | CIN I | CIN II, CIN III |
| Very old terminology | mild dysplasia | moderate dysplasia, severe dysplasia |
Treatment
Overview:
- LSIL: follow-up unless persistent. It usually regresses on its own.
Microscopic
Features:[1]
- "Koilocytic atypia":[2]
Note:
- Atypical cells usually close to basement membrane.
- May be seen, focally, in the upper layers.[2]
DDx:
Koilocytes versus benign squamous
Koilocytes:
- Perinuclear clearing.
- Nuclear changes.
- Size similar (or larger) to those in the basal layer of the epithelium.
- Nuclear enlargement should be evident on low power, i.e. 25x. [4]
- Central location - nucleus should be smack in the middle of the cell.
Notes:
- Both perinuclear clearing and nuclear changes are essential.
- Benign cells have a small nucleus that is peripheral.
Images
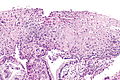
LSIL - intermed. mag. (WC)

LSIL - intermed. mag. (WC)

LSIL - high mag. (WC)

LSIL - very high mag. (WC)




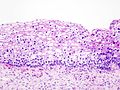
CIN I. (WC/KGH)
_koilocytosis.jpg)
www:
IHC
Features:[5]
- p16.
- Diffuse strong staining involving at least all of the basal aspect of the epithelium = CIN II or CIN III.
- Patchy, weak positive staining = CIN I or squamous metaplasia.
- Ki-67.
- Several positive cells above basal layer suggests CIN II or CIN III.
Notes:
- Both p16 and Ki-67 are usually negative in CIN I -- 75% of cases.[6]
- CIN I with p16 staining appears to have a higher risk of progression the p16 negative CIN I.[7]
See also
References
- ↑ Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 1075-6. ISBN 0-7216-0187-1.
- ↑ Jump up to: 2.0 2.1 Nucci, Marisa R.; Oliva, Esther (2009). Gynecologic Pathology: A Volume in Foundations in Diagnostic Pathology Series (1st ed.). Churchill Livingstone. pp. 146. ISBN 978-0443069208.
- ↑ Roteli-Martins CM, Derchain SF, Martinez EZ, Siqueira SA, Alves VA, Syrjänen KJ (2001). "Morphological diagnosis of HPV lesions and cervical intraepithelial neoplasia (CIN) is highly reproducible". Clin Exp Obstet Gynecol 28 (2): 78–80. PMID 11491378.
- ↑ V. Dube 2008.
- ↑ Singh, M.; Mockler, D.; Akalin, A.; Burke, S.; Shroyer, A.; Shroyer, KR. (Feb 2012). "Immunocytochemical colocalization of P16(INK4a) and Ki-67 predicts CIN2/3 and AIS/adenocarcinoma.". Cancer Cytopathol 120 (1): 26-34. doi:10.1002/cncy.20188. PMID 22162342.
- ↑ Jackson, JA.; Kapur, U.; Erşahin, Ç. (Apr 2012). "Utility of p16, Ki-67, and HPV test in diagnosis of cervical intraepithelial neoplasia and atrophy in women older than 50 years with 3- to 7-year follow-up.". Int J Surg Pathol 20 (2): 146-53. doi:10.1177/1066896911427703. PMID 22104735.
- ↑ del Pino, M.; Garcia, S.; Fusté, V.; Alonso, I.; Fusté, P.; Torné, A.; Ordi, J. (Nov 2009). "Value of p16(INK4a) as a marker of progression/regression in cervical intraepithelial neoplasia grade 1.". Am J Obstet Gynecol 201 (5): 488.e1-7. doi:10.1016/j.ajog.2009.05.046. PMID 19683687.