Difference between revisions of "Dermal cysts"
| Line 77: | Line 77: | ||
====Micro==== | ====Micro==== | ||
The sections show hair-bearing skin with a cyst that is lined by squamous epithelium with a granular layer. The cyst contains keratin. The overlying epithelium is unremarkable. | The sections show hair-bearing skin with a cyst that is lined by squamous epithelium with a granular layer. The cyst contains keratin. The overlying epithelium is unremarkable. | ||
=====Ruptured===== | |||
The section shows a dermal collection of neutrophils with acellular keratin-like material surrounded by histiocytes and fibrosis. The lesion is completely excised in the plane of section. Hair follicles are adjacent to the abscess; however, they are not inflamed. | |||
==Pilar cyst== | ==Pilar cyst== | ||
Revision as of 22:03, 24 September 2012
Dermal cysts, also skin cysts, are common in dermatopathology. Dermatopathologists can diagnose 'em.
Cysts
Common types:[1]
- Epidermal cyst (sebaceous cyst) -- most common.
- Pilar (trichilemmal) cyst.
- Dermoid cyst.
- Ganglion cyst.
- Milicem.
Epidermal necrosis
- This may be cystic. It is covered in the epidermal necrosis article, which covers erythema multiforme, Steven-Johnson syndrome and toxic epidermal necrolysis.
Venous lake
General
- Dilated vein.
Clinical:
- Blanch with pressure.[2]
Gross
- Purple/blue spot.
Images:
Microscopic
Features:[4]
- Lined by endothelium.
- Blood in lumen.
- +/-Fibrin in lumen.
- +/-Solar elastosis - very common.[5]
DDx:
- Angiokeratoma.
- Ectatic superficial dermal vessels.
- Irregular acanthosis.
- Longer rete ridges.
- Cherry hemangioma.[5]
Images:
Epidermal inclusion cyst
General
- Very common.
Microscopic
Features:
- Cyst lining has a granular layer - key feature.[7]
- Trapped collagen bundles at edge of lesion with surrounded by fibroblasts.
- Keratin.
- +/-Granulomatous inflammation due to rupture.
Image:
DDx:
- Pilar cyst - no granular layer.
- Eccrine hidrocystoma - eyelid lesion; same histology.[9]
- Dermoid cyst - has adnexal structures, i.e. hair follicle, sebaceous glands, sweat glands.
- Cystic squamous cell carcinoma.[10]
- Keratoacanthoma.[6]
- Dermatofibrosarcoma protuberans - if lesion is large.
Sign out
SKIN CYST, BACK, EXCISION: - EPIDERMAL INCLUSION CYST.
Micro
The sections show hair-bearing skin with a cyst that is lined by squamous epithelium with a granular layer. The cyst contains keratin. The overlying epithelium is unremarkable.
Ruptured
The section shows a dermal collection of neutrophils with acellular keratin-like material surrounded by histiocytes and fibrosis. The lesion is completely excised in the plane of section. Hair follicles are adjacent to the abscess; however, they are not inflamed.
Pilar cyst
- AKA trichilemmal cyst.
General
- Very common.
Gross
- Classic location: head ~90%.[11]
Microscopic
Features:
- Keratin.
- Cyst lining has no granular layer - key feature.
- Trapped collagen bundles at edge of lesion with surrounded by fibroblasts.
DDx:
- Epidermal cyst - has a granular layer.
Images:
- www:
- WC:
{kind=link}
{kind=link}
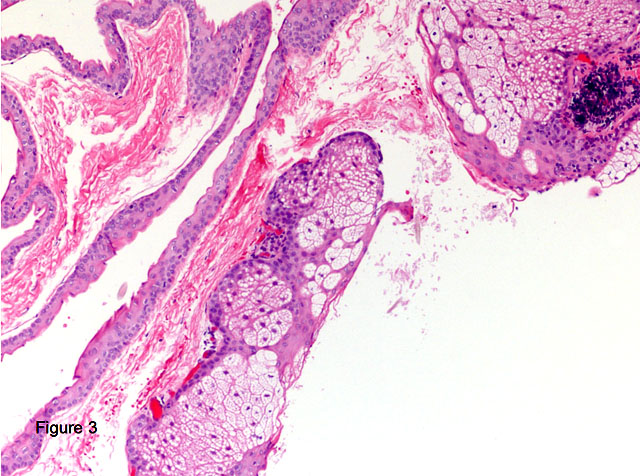
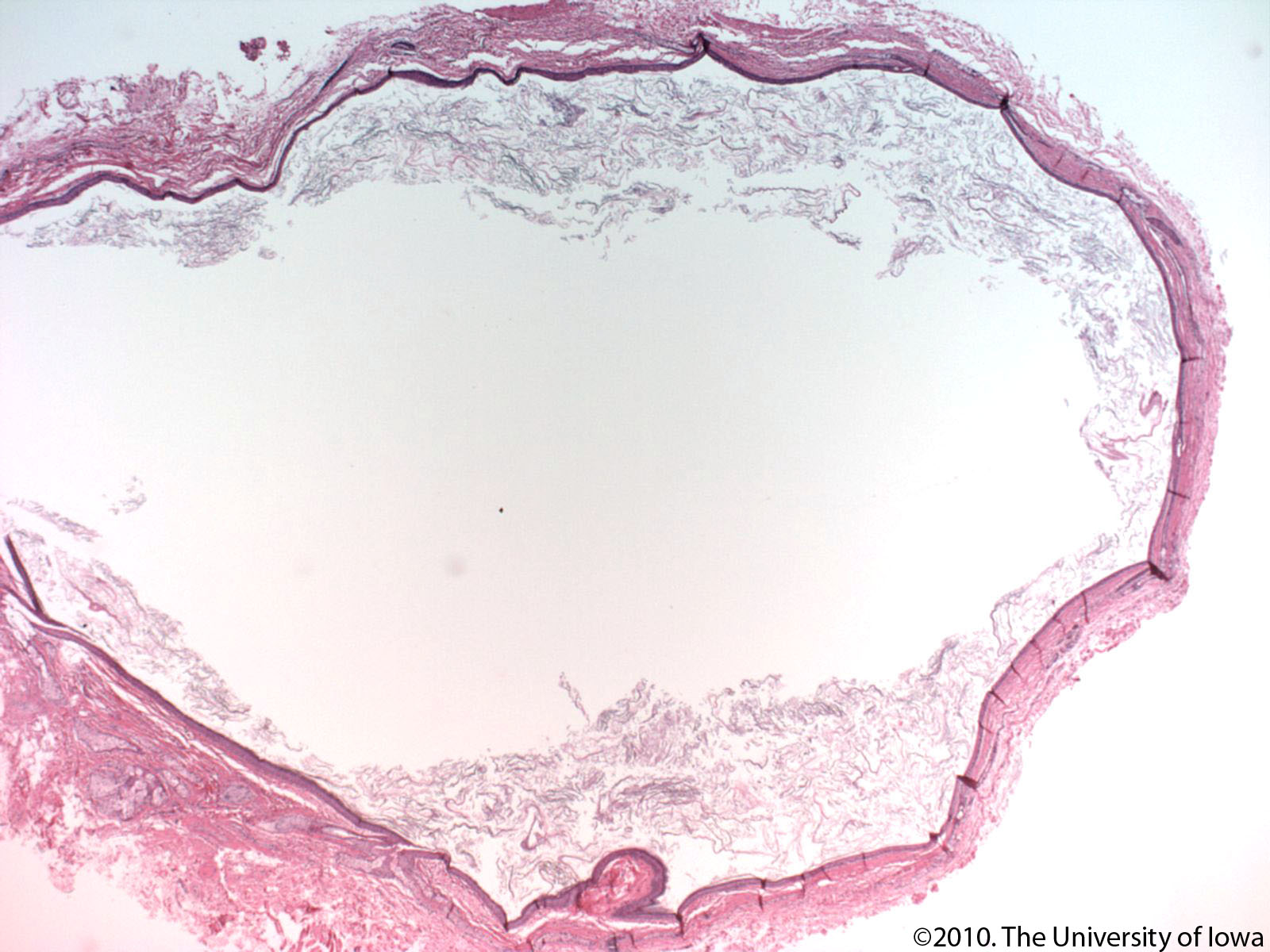
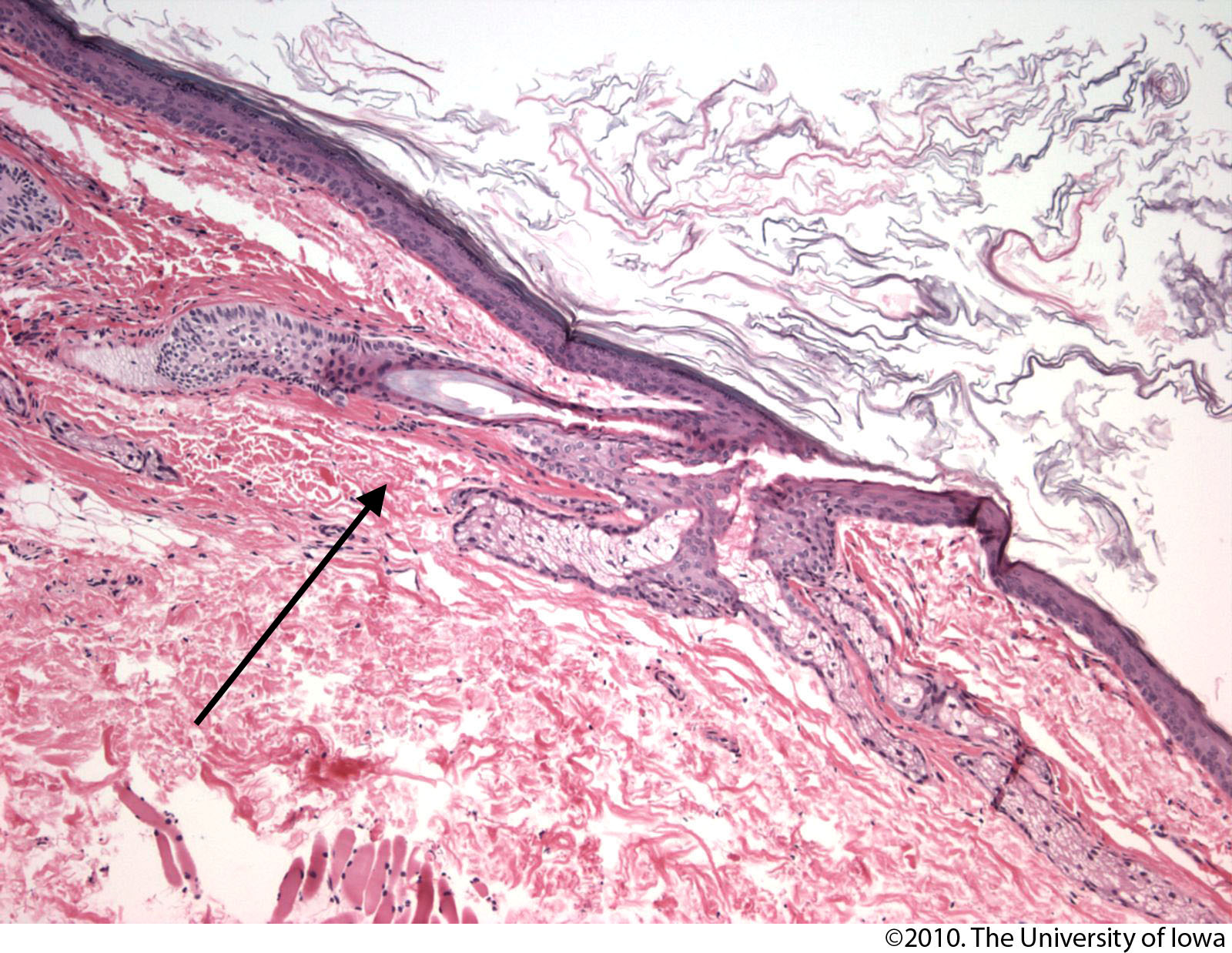
Steatocystoma
General
- Benign.
- Typically adults.
- Usually on the trunk.
- May be genetic; known as steatocystoma multiplex.[12]
- Classically autosomal dominant.[13]
Microscopic
Features:[14]
- Cyst lined by squamous epithelium with:
- Corrugated eosinophilic lining - key feature.
- Similar appearance to compact keratin (hyperkeratosis).
- Described as a hyaline cuticle.[15]
- No granular cell layer.
- Corrugated eosinophilic lining - key feature.
Images:
- www:
- WC:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Dermoid cyst
General
- Benign.
- Congenital choristomas.[17]
- May be found in the ovary.
Microscopic
- Cyst lined by normal (keratinized) skin with adnexal structure (hair follicles, sweat glands, sebaceous glands).
DDx:
- Epidermal cyst - no adnexal structures.
Images:
{kind=link}
{kind=link}
Digital mucous cyst
General
- Dome-shaped papule.
Microscopic
Features:[19]
- Mucous in superficial dermis - key feature.
- No epithelial lining; it is a pseudocyst.
Note:
- Mucin = glycolated proteins; may be part of mucous.
- Mucous = slippery secretion.
DDx:
Images:
{kind=link}
Pilonidal cyst
General
- Benign.
- Young adults (late teens, early twenties) - usu. men.[23]
Gross
- Usually at gluteal folds.
- Uncommon: axilla, genital region, umbilicus, scalp.[24]
Microscopic
Features:[24]
- Cyst or pseudocyst into the deep dermis.
- May be lined by squamous epithelium with inflammation +/-pseudoepitheliomatous hyperplasia.
- Neutrophils.
- Granulomatous inflammation.
DDx:
- Squamous cell carcinoma of the skin with inflammation.[25]
- Infection.
Sign out
SKIN LESION (PILONIDAL SINUS), EXCISION: - PILONIDAL SINUS. - NEGATIVE FOR MALIGNANCY.
Micro
The section shows hair-bearing skin with a deep sinus tract containing large clusters of neutrophils, abundant plasma cells, hemosiderin-laden macrophages, eosinophils and multinucleated giant cells. The core of the lesion is, focally, well-vascularized. At the edge of the lesion is fibrotic tissue with plump fibroblasts. Benign, fibrofatty tissue with scant inflammation completely surrounds the tract, in the plane of section; however, it is focally fragmented. There is no squamous lining within the sinus. No nuclear atypia is identified.
See also
References
- ↑ Greenwald, J.; Heng, M. (2007). Toronto Notes for Medical Students 2007 (2007 ed.). The Toronto Notes Inc. for Medical Students Inc.. pp. D5. ISBN 978-0968592878.
- ↑ URL: http://dermatlas.med.jhmi.edu/derm/IndexDisplay.cfm?ImageID=-969536424. Accessed on: 13 August 2012.
- ↑ 3.0 3.1 3.2 URL: http://dermatlas.med.jhmi.edu/derm/result.cfm?Diagnosis=605386295. Accessed on: 13 August 2012.
- ↑ Weedon's Skin Pathology. 3rd Ed. P.895.
- ↑ 5.0 5.1 Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 551. ISBN 978-0443066542.
- ↑ 6.0 6.1 Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 302. ISBN 978-0443066542.
- ↑ URL: http://emedicine.medscape.com/article/1058907-diagnosis. Accessed on: 18 March 2011.
- ↑ Crystal, P.; Shaco-Levy, R. (Mar 2005). "Concentric rings within a breast mass on sonography: lamellated keratin in an epidermal inclusion cyst.". AJR Am J Roentgenol 184 (3 Suppl): S47-8. PMID 15728019.
- ↑ Adams, SP. (Feb 1999). "Dermacase. Eccrine hydrocystoma.". Can Fam Physician 45: 297, 306. PMC 2328272. PMID 10065300. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2328272/.
- ↑ Lin, CY.; Jwo, SC. (Apr 2002). "Squamous cell carcinoma arising in an epidermal inclusion cyst.". Chang Gung Med J 25 (4): 279-82. PMID 12079164.
- ↑ URL: http://emedicine.medscape.com/article/1058907-overview. Accessed on: 15 April 2012.
- ↑ Online 'Mendelian Inheritance in Man' (OMIM) 184500
- ↑ URL: http://path.upmc.edu/cases/case674/dx.html. Accessed on: 29 January 2012.
- ↑ Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 312. ISBN 978-0443066542.
- ↑ URL: http://path.upmc.edu/cases/case674/dx.html. Accessed on: 29 January 2012.
- ↑ URL: http://path.upmc.edu/cases/case674.html. Accessed on: 29 January 2012.
- ↑ 17.0 17.1 17.2 Gandhi N, Syed NA, Alen R. Dermoid Cyst. EyeRounds.org. posted July 26, 2010; Available from: http://www.EyeRounds.org/cases/115-dermoid-cyst.htm. Accessed on: 22 September 2011.
- ↑ Mitchell, Richard; Kumar, Vinay; Fausto, Nelson; Abbas, Abul K.; Aster, Jon (2011). Pocket Companion to Robbins & Cotran Pathologic Basis of Disease (8th ed.). Elsevier Saunders. pp. 596. ISBN 978-1416054542.
- ↑ 19.0 19.1 URL: http://www.dermpedia.org/dermpedia-textbook/digital-mucous-myxoid-cyst. Accessed on: 17 January 2012.
- ↑ URL: http://dictionary.reference.com/browse/mucous. Accessed on: 8 January 2012.
- ↑ URL: http://dictionary.reference.com/browse/mucus. Accessed on: 8 January 2012.
- ↑ URL: http://emedicine.medscape.com/article/788127-overview. Accessed on: 10 September 2012.
- ↑ URL: http://www.nhs.uk/conditions/Pilonidal-sinus/Pages/Introduction.aspx. Accessed on: 10 September 2012.
- ↑ 24.0 24.1 Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 326. ISBN 978-0443066542.
- ↑ Chatzis, I.; Noussios, G.; Katsourakis, A.; Chatzitheoklitos, E.. "Squamous cell carcinoma related to long standing pilonidal-disease.". Eur J Dermatol 19 (4): 408-9. doi:10.1684/ejd.2009.0705. PMID 19482585.