Cholestasis
(Redirected from Cholestatic hepatitis)
Jump to navigation
Jump to search
Error creating thumbnail:
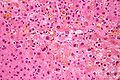
Micrograph showing cholestasis, as is apparent by the yellow bile. H&E stain. (WC)
In liver pathology, cholestasis is a stoppage or abnormally slow flow of bile.
Cholestatic hepatitis and feathery degeneration redirect to this article.
General
Clinical - classic:[1]
- Dark urine and light stools.
Short DDx - by etiology
- Congenital: Bile duct cyst, biliary atresia, liver cysts.
- Infectious: Worm.
- Tumour: pancreas, bile duct, liver.
- Endocrine: cholestasis of pregnancy.
- Trauma -> sepsis.
- Autoimmune: PSC, PBC.
- Toxins: alcohol -> cirrhosis.
- Everything else: drugs, e.g. NSAIDs.
Short DDx - structural
- Obstruction - large duct:
- Tumour.
- Gallstone.
- Worm.
- PSC.
- Small duct - autoimmune:
- PBC.
- Other:
- Rx.
- Toxins.
- Cholestasis of pregnancy.
Microscopic
Appearance of bile:
- Smooth/homogenous.
- Brown/yellow.
- Globule/droplet - that is larger than an iron granule.
Note:
- Iron in bile ducts or endothelial cell = non-specific, used to be thought to be specific for hereditary hemochromatosis.
Brown/yellow cytoplasmic inclusions
Comparison of brown/yellow cytoplasmic inclusions:[2]
| Finding | Colour | Granularity | Refractile | Usual location | Association | Stain | Image |
|---|---|---|---|---|---|---|---|
| Iron | Brown | Coarse granules | Yes - shinny | Periportal (zone I) |
Hemolysis, hereditary hemochromatosis | Prussian blue +ve | File:Sickle cell disease and cirrhosis - very high mag.jpg Iron and bile. (WC) |
| Bile | Brown - coffee stained | Not granular | No - dull | Portal | Duct injury/obstruction | None | Error creating thumbnail: Bile. (WC) |
| Lipofuscin | Yellow | Fine granules | No | Centrilobular (zone III) |
Advanced age | PAS stain +ve | File:Ground glass hepatocytes high mag cropped.jpg Lipofuscin. (WC) |
Large duct obstruction
Histologic findings of large-duct obstruction:[3]
- Perivenular bilirubinostasis.
- Portal tract edema & inflammation (neutrophils & macrophages).
- Large bile plugs.
- Bile duct proliferation.[4][5]
Note:
- Ductular reaction = increased number of ducts + neutrophils.[6]
Small duct obstruction
Small-duct obstruction:
- Abnormal liver plate architecture. (???)
Images
Cholestasis. (WC/Nephron)

{kind=link}
{kind=link}
www:
Sign out
LIVER, CORE BIOPSY: - CENTRILOBULAR CHOLESTATSIS (MILD), SEE MICROSCOPIC DESCRIPTION AND COMMENT. - NEGATIVE FOR FIBROSIS. COMMENT: There is no apparent feathery degeneration. There is no bile ductular proliferation. No definite onion-skin lesions are identified. The centrilobular distribution of the bile favours a large duct obstruction. Possible causes include gallstones, other obstructing lesions, herbals and drugs. Clinical and radiologic correlation is suggested.
See also
References
- ↑ URL: http://www.patient.co.uk/doctor/cholestasis. Accessed on: 28 November 2013.
- ↑ Guindi, M. September 2009.
- ↑ Burt, Alastair D.;Portmann, Bernard C.;Ferrell, Linda D. (2006). MacSween's Pathology of the Liver (5th ed.). Churchill Livingstone. pp. 565. ISBN 978-0-443-10012-3.
- ↑ Chapman RW, Arborgh BA, Rhodes JM, et al. (October 1980). "Primary sclerosing cholangitis: a review of its clinical features, cholangiography, and hepatic histology". Gut 21 (10): 870–7. PMC 1419383. PMID 7439807. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1419383/.
- ↑ Leuschner U (November 2003). "Primary biliary cirrhosis--presentation and diagnosis". Clin Liver Dis 7 (4): 741–58. PMID 14594129.
- ↑ Roskams, T.; Desmet, V. (Nov 1998). "Ductular reaction and its diagnostic significance.". Semin Diagn Pathol 15 (4): 259-69. PMID 9845427.