Pilomatricoma
| Pilomatricoma | |
|---|---|
| Diagnosis in short | |
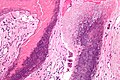
 Pilomatricoma. H&E stain. | |
|
| |
| LM | "ghost" cells, foreign body-type giant cells |
| LM DDx | squamous cell carcinoma, pilomatrix carcinoma, basal cell carcinoma, epidermal inclusion cyst, heterotopic ossification |
| Gross | skin nodule, hard |
| Site | skin |
|
| |
| Clinical history | common in children |
| Signs | hard nodule |
| Symptoms | +/-painful |
| Prevalence | common |
| Prognosis | benign |
| Clin. DDx | surgical excision |
Pilomatricoma is a benign skin lesion that is common in childhood. It may be spelled pilomatrixoma.
It is also known as calcifying epithelioma of Malherbe.[1]
General
- Benign skin tumour.
- Most common solid skin tumour of children.[2]
- CTNNB1 gene mutation important in pathogenesis.[3]
Clinical:
- Hard nodule - calcification.
- +/-Painful.
Treatment:
- Surgical excision.[2]
Microscopic
Features:[4]
- Nodular circumscribed lower dermis/subcutaneous adipose lesion; thus, usu. surrounded by connective tissue.
- Sharpy demarcated island of cells.
- Calcification in 75%.
- Cells:[5]
- Basaloid epithelial cells - have prominent nucleoli.
- Anucleate squamous cells ("ghost cells").
- Giant cell foreign body type granulomas (form in reaction to keratin).
Notes:
- Keratin a prominent feature on cytology - lots of orange stuff.
- May (extensively) ossify.[6]
DDx:
- Epidermal inclusion cyst.
- Pilomatrix carcinoma - invasive border, cytologic atypia, necrosis.[7]
- Squamous cell carcinoma.
- Basal cell carcinoma.
- Heterotopic ossification.
Images
Pilomatrixoma - high mag. (WC/Nephron)

Pilomatrixoma - intermed. mag. (WC/Nephron)

www:
Sign out
Skin Lesion, Left Forearm, Excision: - Pilomatricoma with ossification.
Block letters
SKIN LESION, RIGHT ARM, EXCISION: - PILOMATRICOMA.
Micro
The sections show anucleate squamous cells ("ghost cells") and multinucleated giant cells. No calcification is present. No significant nuclear atypia is present. No mitotic activity is apparent. There is also mildly inflamed fibroadipose tissue and some benign squamous mucosa.
Alternate
The sections show anucleate squamous cells ("ghost cells") and multinucleated giant cells. Calcification is present. No significant nuclear atypia is present. No mitotic activity is apparent. The lesion extends to the inked surface. No skin is present.
See also
References
- ↑ Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 387. ISBN 978-0443066542.
- ↑ 2.0 2.1 URL: http://emedicine.medscape.com/article/1058965-overview. Accessed on: 10 September 2011.
- ↑ Mitchell, Richard; Kumar, Vinay; Fausto, Nelson; Abbas, Abul K.; Aster, Jon (2011). Pocket Companion to Robbins & Cotran Pathologic Basis of Disease (8th ed.). Elsevier Saunders. pp. 597. ISBN 978-1416054542.
- ↑ URL: http://emedicine.medscape.com/article/1058965-diagnosis. Accessed on: 10 September 2011.
- ↑ http://www.bccancer.bc.ca/HPI/CE/cytotechnology/cytosleuthquiz/nongyne/ngcase02d.htm
- ↑ Ioannidis, O.; Stavrakis, T.; Cheva, A.; Papadimitriou, N.; Kotronis, A.; Kakoutis, E.; Makrantonakis, N. (2010). "Pilomatricoma of the arm with extensive ossification.". Adv Med Sci 55 (2): 340-2. doi:10.2478/v10039-010-0010-y. PMID 20439187.
- ↑ Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 389. ISBN 978-0443066542.