Difference between revisions of "Squamous cell carcinoma of the penis"
Jump to navigation
Jump to search
| Line 7: | Line 7: | ||
| Micro = | | Micro = | ||
| Subtypes = | | Subtypes = | ||
| LMDDx = | | LMDDx = [[penile intraepithelial neoplasia]], [[pseudoepitheliomatous hyperplasia]] | ||
| Stains = | | Stains = | ||
| IHC = | | IHC = | ||
Revision as of 07:20, 9 February 2015
| Squamous cell carcinoma of the penis | |
|---|---|
| Diagnosis in short | |
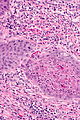
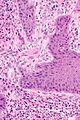
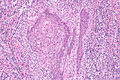
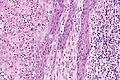
 Squamous carcinoma of the penis. H&E stain. | |
| LM DDx | penile intraepithelial neoplasia, pseudoepitheliomatous hyperplasia |
| Gross | mass lesion, scaly patches/nodules, usu. erythematous, +/-ulceration. |
| Grossing notes | penectomy |
| Site | penis |
|
| |
| Clinical history | uncircumcised |
| Prevalence | uncommon overall, most common form of penis cancer |
| Prognosis | good |
| Treatment | surgery |
Squamous cell carcinoma of the penis is the most common malignancy of the penis.
Penile cancer redirects to this article.
General
- Not very common overall.[1]
- Most common form of penile cancer.
- Non-squamous penis cancer only ~5% of cases.[2]
Epidemiology:[1]
- Median age ~ 67 years old.
- Usually a good outcome - 5 year cause specific survival ~ 81%.[1]
Gross
- Scaly patches/nodules.
- Usually erythematous.
- +/-Ulceration.
Microscopic
Features:
Notes:
- Lymphovascular invasion - prognostically important,[3] and changes the T-stage for pT1a tumours to pT1b.
DDx:
Grading
- G1 - well differentiated. §
- Almost normal appearing - diagnosis of malignancy may be challenging.
- G2 - moderately differentiated. §
- G3 - poorly differentiated.
- Anaplastic cells.
- Typically little or no keratinization.
- GX - cannot be assessed.
Notes:
- § The differentiation between G1 and G2 is similar to squamous cell carcinoma of the head and neck.
- G2 (moderately differentiated) is the most common.[1]
Staging
T-stage:
- pT1a - subepithelial tissue involved, no LVI, not poorly differentiated (G3).
- pT1b - subepithelial tissue involved with LVI or poorly differentiated.
- pT2 - corpus spongiosum or cavernosum involved.
- pT3 - urethral involvement.
- pT4 - adjacent structure(s) involved.
Images

Penile SCC - low mag.
Penile SCC - high mag.
Penile SCC - high mag.
Penile SCC - intermed. mag.
Penile SCC - high mag.




Sign out
Tip of Penis, Partial Penectomy: - Invasive squamous cell carcinoma, moderately differentiated (G2). -- Invasion into the lamina propria. -- Surgical margins negative for dysplasia and negative for malignancy. -- TNM stage: pT1a pNx. -- Please see tumour summary.
All caps
TIP OF PENIS, PARTIAL PENECTOMY: - INVASIVE SQUAMOUS CELL CARCINOMA, MODERATELY DIFFERENTIATED. -- SURGICAL MARGINS NEGATIVE FOR DYSPLASIA AND NEGATIVE FOR MALIGNANCY. -- PLEASE SEE TUMOUR SUMMARY.
TIP OF PENIS, PARTIAL PENECTOMY: - INVASIVE SQUAMOUS CELL CARCINOMA OF CORONAL SULCUS, MODERATELY DIFFERENTIATED. -- SURGICAL MARGINS NEGATIVE FOR DYSPLASIA AND NEGATIVE FOR MALIGNANCY. - LICHEN SCLEROSIS. - POST-SURGICAL CHANGES (GRANULOMATOUS INFLAMMATION (NON-NECROTIZING), SIDEROPHAGES). COMMENT: This lesion was previously excised. The surgical clearance is 1 mm. The tumour thickness is approximately 4 mm. No lymphovascular invasion is identified. No lymphovascular invasion is identified. No corpus spongiosum or corpus cavernosum invasion is seen. The staging is unchanged.
See also
References
- ↑ 1.0 1.1 1.2 1.3 Burt, LM.; Shrieve, DC.; Tward, JD. (Jan 2014). "Stage presentation, care patterns, and treatment outcomes for squamous cell carcinoma of the penis.". Int J Radiat Oncol Biol Phys 88 (1): 94-100. doi:10.1016/j.ijrobp.2013.08.013. PMID 24119832.
- ↑ Moses, KA.; Sfakianos, JP.; Winer, A.; Bernstein, M.; Russo, P.; Dalbagni, G. (Dec 2013). "Non-squamous cell carcinoma of the penis: single-center, 15-year experience.". World J Urol. doi:10.1007/s00345-013-1216-y. PMID 24292119.
- ↑ Bhagat, SK.; Gopalakrishnan, G.; Kekre, NS.; Chacko, NK.; Kumar, S.; Manipadam, MT.; Samuel, P. (Feb 2010). "Factors predicting inguinal node metastasis in squamous cell cancer of penis.". World J Urol 28 (1): 93-8. doi:10.1007/s00345-009-0421-1. PMID 19488760.