Difference between revisions of "Seborrheic keratosis"
(→Micro) |
|||
| Line 117: | Line 117: | ||
===Micro=== | ===Micro=== | ||
The sections show skin with acanthosis, pseudohorn cysts | The sections show skin with acanthosis, pseudohorn cysts, hyperkeratosis and focal basal epidermal pigmentation. There is no basal nuclear atypia, and there are no | ||
melanocytic nests. Mitotic activity is not apparent. There is minimal dermal inflammation. There is no apparent solar elastosis. | melanocytic nests. Mitotic activity is not apparent. There is minimal dermal inflammation. There is no apparent solar elastosis. | ||
| Line 135: | Line 135: | ||
There is no hyperkeratosis or acanthosis. No pigmentation is apparent. No large blood | There is no hyperkeratosis or acanthosis. No pigmentation is apparent. No large blood | ||
vessels are identified. No nuclear atypia is seen. | vessels are identified. No nuclear atypia is seen. | ||
====Irritated SK==== | |||
The sections show skin with acanthosis, pseudohorn cysts, hyperkeratosis and basal epidermal pigmentation. There are no melanocytic nests. Mitotic activity is not readily apparent. A dermal lymphohistiocytic infiltrate is present. Reactive basal cell changes are present. There is no apparent solar elastosis. The lesion is incompletely | |||
excised. | |||
==See also== | ==See also== | ||
Revision as of 16:57, 11 October 2013
| Seborrheic keratosis | |
|---|---|
| Diagnosis in short | |
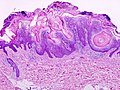
.jpg) Seborrheic keratosis. H&E stain. | |
|
| |
| LM | horn cysts, pigmented basal layer, hyperkeratosis |
| Subtypes | acanthotic seborrheic keratosis, reticulated seborrheic keratosis, irritated seborrheic keratosis, digitated seborrheic keratosis, stucco keratosis |
| LM DDx |
actinic keratosis, verruca vulgaris, basal cell carcinoma (fibroepitheliomatous pattern) - for reticulated SK, melanocytic nevus, condyloma acuminatum, inverted follicular keratosis |
| Gross | raised lesion |
| Site | skin |
|
| |
| Associated Dx | internal malignancy - if very many |
| Clinical history | old age |
| Prevalence | very common |
| Prognosis | benign |
| Clin. DDx | melanocytic lesion |
Seborrheic keratosis, abbreviated SK, is a very common diagnosis is dermatopathology.
General
- Benign.
- Most common tumour in older people.[1]
- "Large number" of SKs = paraneoplastic syndrome (Leser–Trélat sign).[2]
Epidemiology:
- Old people.
- Usually in sun exposed area.[3]
Gross
- "Stuck-on" appearance - raised lesion.
Image(s):
Microscopic
Features:[2]
- Raised above skin surface.
- Border sharply demarcated.
- Hyperkeratosis - stratum corneum extra thick.
- May be minimal.
- Horn cysts - intraepidermal collections of keratin - key feature.
- Actually invaginations - not true cysts; thus, they may more accurately be called pseudohorn cysts.[4]
- Clusters of cells with brown granular material in the superficial dermis/dermoepidermal junction - pigmented melanocytes.
DDx:[5]
- Actinic keratosis - especially, irritated SKs; have nuclear atypia and parakeratosis.
- Verruca vulgaris - SK may have papillomatous projections.
- Basal cell carcinoma, fibroepitheliomatous pattern - esp. reticulated SK.
- Melanocytic nevus.
- Condyloma acuminatum - may have horn cysts, more probable than SK in the genital area.
- Inverted follicular keratosis - predominantly endophytic growth pattern, may be considered a variant of seborrheic keratosis.[6]
- Collision with another lesion.
- Papillomatous compound nevus - a beign nevus with seborrheic keratosis-like features.
- Acanthosis nigricans - site important.
Images
Seborrheic keratosis - low mag. (WC)

Seborrheic keratosis - high mag. (WC)
.jpg)
www:
- Seborrheic keratosis - high mag. (dermatlas.org).
- Seborrheic keratosis - low mag. (dermatlas.org).
- Gallery of SK variants (ispub.com).
- Acantholytic SK (ispub.com).
Histologic subtypes
Like very common lesion, there are subtypes:[5]
- Acanthotic seborrheic keratosis - thickened stratum spinosum; thick epidermis.
- Reticulated seborrheic keratosis - vaguely resembles fibroepithelioma of Pinkus (BCC, fibroepitheliomatous pattern).
- Irritated seborrheic keratosis - spongiosis (epidermal intercellular edema) and inflammation.
- Digitated seborrheic keratosis - papillomatous projections, architecture mimics a verruca.
- Stucco keratosis - pointed papillomatous projections.
Sign out
SKIN LESION, MID BACK, BIOPSY: - SEBORRHEIC KERATOSIS.
SKIN LESION, RIGHT SCAPULA, PUNCH BIOPSY: - RETICULATED SEBORRHEIC KERATOSIS.
SKIN LESION ("NEVUS"), RIGHT TRUNK AT BRA LINE, SHAVE BIOPSY:
- IRRITATED SEBORRHEIC KERATOSIS (HYPERKERATOTIC TYPE).
SKIN LESION, LEFT POSTERIOR SHOULDER, EXCISION: - SEBORRHEIC KERATOSIS (ACANTHOTIC TYPE), COMPLETELY EXCISED.
SKIN LESION, LEFT POSTERIOR SHOULDER, EXCISION: - SEBORRHEIC KERATOSIS WITH PIGMENTATION (ACANTHOTIC TYPE), COMPLETELY EXCISED IN THE PLANE OF SECTION. - NEGATIVE FOR MELANOCYTIC LESION.
Micro
The sections show skin with acanthosis, pseudohorn cysts, hyperkeratosis and focal basal epidermal pigmentation. There is no basal nuclear atypia, and there are no melanocytic nests. Mitotic activity is not apparent. There is minimal dermal inflammation. There is no apparent solar elastosis.
Without horn pseudocysts
The sections show skin with acanthosis, a thin layer of compact keratin and focal basal epidermal pigmentation. Dilated blood vessels surrounded by collagen are seen in the superficial dermis. No pseudohorn cysts are identified. A granular layer is present.
There is no basal nuclear atypia. There is no mitotic activity and no melanocytic nests. There is no solar elastosis. No koilocytes are apparent.
Minimal hyperkeratosis
The sections show skin with acanthosis, pseudohorn cysts, rare parakeratosis, minimal hyperkeratosis and focal basal epidermal pigmentation. There is no basal nuclear atypia, no appreciable mitotic activity and there are no melanocytic nests. There is minimal dermal inflammation. Solar elastosis is present.
Reticulated seborrheic keratosis
The sections show hair-bearing skin with fine strands of benign basaloid epidermal cells extending from the epidermis. The superficial dermis has dense collagen. No significant inflammation is present. Pseudohorn cysts are present focally.
There is no hyperkeratosis or acanthosis. No pigmentation is apparent. No large blood vessels are identified. No nuclear atypia is seen.
Irritated SK
The sections show skin with acanthosis, pseudohorn cysts, hyperkeratosis and basal epidermal pigmentation. There are no melanocytic nests. Mitotic activity is not readily apparent. A dermal lymphohistiocytic infiltrate is present. Reactive basal cell changes are present. There is no apparent solar elastosis. The lesion is incompletely excised.
See also
References
- ↑ URL: http://emedicine.medscape.com/article/1059477-overview#a0199. Accessed on: 26 August 2011.
- ↑ 2.0 2.1 Mitchell, Richard; Kumar, Vinay; Fausto, Nelson; Abbas, Abul K.; Aster, Jon (2011). Pocket Companion to Robbins & Cotran Pathologic Basis of Disease (8th ed.). Elsevier Saunders. pp. 595. ISBN 978-1416054542.
- ↑ URL: http://emedicine.medscape.com/article/1059477-overview. Accessed on: 26 August 2011.
- ↑ URL: http://www.healthcare.uiowa.edu/dermatology/dpt/HornCyst.htm. Accessed on: 13 September 2012.
- ↑ 5.0 5.1 Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 338-9. ISBN 978-0443066542.
- ↑ Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 341. ISBN 978-0443066542.
- ↑ Lim, C. (May 2006). "Seborrhoeic keratoses with associated lesions: a retrospective analysis of 85 lesions.". Australas J Dermatol 47 (2): 109-13. doi:10.1111/j.1440-0960.2006.00258.x. PMID 16637806.
- ↑ Defazio, J.; Zalaudek, I.; Busam, KJ.; Cota, C.; Marghoob, A. (Apr 2012). "Association between melanocytic neoplasms and seborrheic keratosis: more than a coincidental collision?". Dermatol Pract Concept 2 (2): 202a09. doi:10.5826/dpc.0202a09. PMID 23785597.