Pulmonary pathology
The lung is a forgotten organ in pathology, 'cause radiologists can diagnose much with high resolution CT (HRCT) and a bit of history. This article introduces the lung, discusses an approach to the lung, and the tumours that afflicit it. Medical lung disease is dealt with in the medical lung disease article.
Basic approach
All lung pathology can be grouped into one of six categories (as per Leslie). The radiology directly correlates to the pathologic grouping, except that air space disease encompasses three pathologic categories (ALI, CCI, AFD).
Pathologic groups:
| Lung pathology | |||||||||||||||||||||||||||||||||||||||||||||||
| Acute lung injury | Fibrosis | Chronic cellular infiltrates (ALI) | Alveolar filling defect (AFD) | Nodules | Near normal histology | ||||||||||||||||||||||||||||||||||||||||||
Identification of the groups:
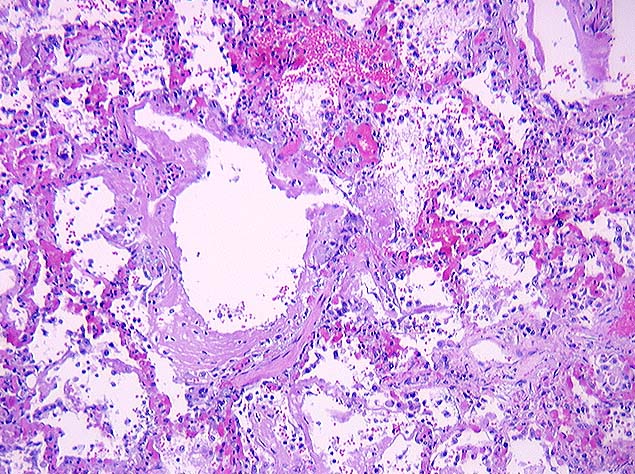
- Acute lung injury: hyaline membranes (very pink on H&E).
- Fibrosis = thick walls - pink on H&E.
- Chronic cellular infiltrates = inflammation (blue on H&E).
- Nodules = look at the history/radiology - should say mass or nodule.
- Alveolar filling defect = crap in the alveoli.
- Near normal = looks almost normal.
Radiologic groups:
| Lung radiology | |||||||||||||||||||||||||||||||
| Air space disease | Interstitial disease | Mass/nodules | Near normal | ||||||||||||||||||||||||||||
Radiologic-pathologic correlation:
- Air space disease (radiologic).
- Acute lung injury.
- Chronic cellular infiltrates.
- Alveolar filling defects.
- Interstitial disease (radiologic).
- Fibrosis.
- Mass/nodules (radiologic).
- Nodules.
- Near normal (radiologic).
- Near normal histology.
Most of the things that come to pathology are in the mass/nodules category and lung tumours (discussed below). The other categories are dealt with in the medical lung disease article.
Normal histology
Cells
- Type I pneumocyte - cover most of the alveolar surface.
- Type II pneumocyte - stem cell, produce surfactant.
- Typical location: "angle of alveolus".
- Macrophages.
Lung lobule
Lung lobule:[1]
- Arterial vessels travels with the bronchus.
- Venules travel in the septae.
- Arterial vessels in the lung should be approximately the same size as its accompanying airway.[2]
Memory device: arteries (which were once thought to contain air) are with the airway.
Small airways
The trip to the alveolus:[3]
- Membranous bronchiole.
- Terminal bronchiole - dilation distal to this = emphysema.
- Respiratory bronchiole.
- Alveolar duct - dilated in ARDS.
- Alveolus.
Anatomy - terms
- Bronchus = has cartilage.
- Bronchiole = non-cartilaginous airway.
Pathology terminology
- Siderophages = mononuclear phagocyte with hemosiderin.[4]
- Hyaline membrane = glassy layering of an alveolus/small airways with material that is eosinophilic on H&E.[5]
- Entomology of Hyaline: "... of glass" (Greek).
- Image: Hyaline membrane (path.upmc.edu).
{kind=link}
- Bronchiolization = ciliated (respiratory) epithelium or goblet cells in (distal) air space.[6]
- Image: Bronchiolization (ucsf.edu).
{kind=link}
- Smoker's macrophages = brown-pigmented macrophages - assoc. with smoking.[7]
Malignancy - lung cancer
This often comes to the pathologist.
Medical lung disease
Includes discussion of things like acute infectious pneumonia and idiopathic pulmonary fibrosis.
Bronchogenic cyst
- Benign.
- Usually in mediastinum.
Microscopy
Features:[8]
- Cyst lined by respiratory epithelium.
Image:
{kind=link}
See also
References
- ↑ http://lib.hku.hk/denlib/exhibition/rarebook/mouth_hygiene_plate.jpg
- ↑ PPP P.266.
- ↑ Hegele. 27 October 2009.
- ↑ http://medical-dictionary.thefreedictionary.com/siderophore
- ↑ http://medical-dictionary.thefreedictionary.com/hyaline+membrane
- ↑ http://pathhsw5m54.ucsf.edu/case27/image277.html
- ↑ PPP P.236.
- ↑ http://asianannals.ctsnetjournals.org/cgi/content/full/16/3/246/F3
{kind=link}