Difference between revisions of "Products of conception"
| Line 231: | Line 231: | ||
The lack of chorionic villi on pathology is a discordance with the clinical findings. | The lack of chorionic villi on pathology is a discordance with the clinical findings. | ||
A non-exhaustive list possible explanations include: non-removal/retension and prior spontaneous passing. Clinical correlation is required. | A non-exhaustive list of possible explanations include: non-removal/retension and prior spontaneous passing. Clinical correlation is required. | ||
</pre> | </pre> | ||
Revision as of 16:11, 5 April 2022
Products of conception, abbreviated POC, is stuff formed from the union of egg and sperm. This article covers POC superficially.
There are separate articles for chorionic villi and gestational trophoblastic disease.
General
Clinical
- Therapeutic abortions - may be abbreviated "MVC" (manual vacuum aspiration).[1]
- Diagnosis of pregnancy: beta-hCG > 10 mIU/mL.
- Beta-hCG calculator: http://www.countdowntopregnancy.com/tools/beta_doubling_calculator.php.
- If the beta-hCG is >1500 mIU/mL -- there is a good chance an ultrasound is diagnostic.[2]
Screening tests
First trimester screen
- PAPP-A.
- Nuchal translucency.
- Beta-hCG.
Maternal serum screen
- Alpha-fetoprotein.
- Beta-hCG.
- Estriol.
Diagnostic tests
- Chorionic villus sampling (10-12 weeks???).
- Amniocentesis (15-16 weeks+).
Microscopic
Features:
- Chorionic villi are need to call POC - key feature.
- Cytotrophoblast.
- Centre of villi often have fetal red blood cells (which have nuclei) -- not required for diagnosis of POC.
- +/-Endometrium (intrauterine pregnancy):
- Should have decidual changes -- mnemonic NEW:
- Nucleus central.
- Eosinophilic cytoplasm.
- Well-defined cell borders.
- Should have decidual changes -- mnemonic NEW:
- +/-Uterine tube +/- decidualization (tubal pregnancy).
- +/-Hyaline globules.[3]
- +/-Embryo or fetus - a bonus.
- Cartilage - common.
- Primitive neuroepithelium.
- Gastrointestinal epithelium.
Aside:
- Embryo = conceptus before 8 weeks.
- Fetus = conceptus 8th weeks 'til birth.
DDx:
Images
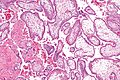
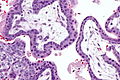
Chorionic villi - intermed. mag. (WC)

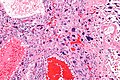
Chorionic villi and fetal parts - low mag. (WC)



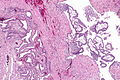
Intermediate trophoblast reaction - low mag. (WC)
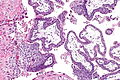
Intermediate trophoblast - high mag. (WC)


www:
Specific conditions
Arias-Stella reaction
General
- Benign atypical endometrial changes associated with chorionic tissue.[4]
- May be seen in a normal pregnancy, hydatidiform moles, others.
- Historically it was diagnosed as endometrial cancer.
Note:
- To the novice... the nuclei look really scary, i.e. they look like cancer.
Microscopic
Features:[4]
- Epithelial component of endometrium with large nuclei - key feature.
- +/-Nuclear hyperchromasia, i.e. dark nuclei.
- +/-Irregular nuclear membrane.
- +/-Nuclear clearing.[5]
- +/-Nuclear pseudoinclusions.
- NC ratio is preserved.[5]
- Usually a focal change.
- +/-Mitoses - uncommon.
Notes:
- No decidual reaction in the stroma.
DDx:
Images
Subtypes
There are five subtypes:[4]
- Minimal atypia.
- Usually early gestation.
- Early secretory pattern.
- Mimics secretory endometrium: cytoplasmic vacuoles, central nucleus, palisading architecture.
- Secretory or hypersecretory pattern.
- Regenerative, proliferative or nonsecretory pattern.
- Monstrous cell pattern.
Ectopic pregnancy
General
- Chorionic villi have to be identified (in some location, e.g. Fallopian tube) to Dx a pregnancy.
- Endometrium: decidual reaction, as seen in any pregnancy.
Clinical:
- Abdominal pain in woman of childbearing age.
- Every woman of childbearing age should be assumed pregnant until proven otherwise![7]
- Typical gestational age (GA) for a tubal pregnancy ~ 5-9 weeks.[8]
- Beta-hCG elevated but may be relatively low (<100 IU/L) even in the context of (uterine tube) rupture.[8]
Microscopic
- See Microscopic section above.
DDx:
- Hydropic abortus.
- Complete hydatidiform mole.
- Partial hydatidiform mole.
Images
EP - low mag. (WC)
EP - intermed. mag. (WC)
EP - high mag. (WC)
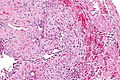
EP - intermed. mag. (WC)




{kind=link}
Sign out
Fallopian Tube, Right Salpingectomy:
- Fallopian tube with chorionic villi (tubal pregnancy).
Submitted as "Left Fallopian Tube and Ectopic Pregnancy", Excision:
- Tubal pregnancy; Fallopian tube with chorionic villi and fetal parts.
Block letters
FALLOPIAN TUBE, RIGHT, SALPINGECTOMY: - FALLOPIAN TUBE WITH CHORIONIC VILLI (TUBAL PREGNANCY).
Micro
The sections show fallopian tube wall with chorionic villi.
Nucleated red blood cells are present. No other fetal components are identified.
The chorionic villi do not show a Norwegian fjord-like periphery. Central cisterns are not apparent. There is no trophoblastic proliferation.
Retained products of conception
General
- May occur in a number of contexts, e.g. therapeutic abortion, sponatenous abortion.
Microscopic
- See Microscopic section above.
DDx:
Sign out
Submitted as "Products of Conception": - Chorionic villi present with degenerative changes, NEGATIVE for proliferation or significant atypia. - Benign decidual tissue present. - Necro-inflammatory debris and fibrin.
Variants
Submitted as "Products of Conception": - Fetal tissue present. - Benign decidual tissue present. - Chorionic villi present, NEGATIVE for proliferation or significant atypia.
Submitted as "Products of Conception": - Chorionic villi present with degenerative changes, negative for proliferation or significant atypia. - Benign decidual tissue present. - Negative for fetal tissue.
Products of Conception, Curettage: - Chorionic villi present without proliferation or significant atypia. - Decidua present. - Negative for malignancy.
No chorionic villi
Submitted as "Products of Conception", Curettage: - Blood and fibrin. - Scant benign squamous epithelium and scant benign endocervical epithelium. - NEGATIVE for decidua. - NEGATIVE for chorionic villi, see comment. Comment: The tissue was submitted in total. Clinical correlation is suggested. The above was communicated to the on call gynecologist.
Notes:
- The above is considered a critical diagnosis.
- It should be communicated to the on call gynecologist and this communication should be documented.
Submitted as "Products of Conception":
- Decidualized endometrium with necro-inflammatory changes/degeneration,
blood and fibrin.
- NEGATIVE for chorionic villi, see comment.
Comment:
The tissue was submitted in total.
The ultrasound impression (intrauterine gestational sac present) is noted. The decrease in serum beta-hCG is noted.
The lack of chorionic villi on pathology is a discordance with the clinical findings.
A non-exhaustive list of possible explanations include: non-removal/retension and prior spontaneous passing. Clinical correlation is required.
Block letters
ENDOMETRIUM, CURETTAGE: - OUTLINES CONSISTENT WITH NON-VIABLE CHORIONIC VILLI WITH FIBRIN AND FOCAL CALCIFICATIONS (COMPATIBLE WITH RETAINED PRODUCTS OF CONCEPTION). - ENDOCERVICITIS, CHRONIC. - NO DEFINITE ENDOMETRIUM. - NO VIABLE CHORIONIC VILLI IDENTIFIED. - NO EVIDENCE OF MALIGNANCY.
See also
References
- ↑ Edelman A, Nichols MD, Jensen J (June 2001). "Comparison of pain and time of procedures with two first-trimester abortion techniques performed by residents and faculty". Am. J. Obstet. Gynecol. 184 (7): 1564-7. PMID 11408881. http://linkinghub.elsevier.com/retrieve/pii/S0002937801372241.
- ↑ Barnhart, KT.; Simhan, H.; Kamelle, SA. (Oct 1999). "Diagnostic accuracy of ultrasound above and below the beta-hCG discriminatory zone.". Obstet Gynecol 94 (4): 583-7. PMID 10511363.
- ↑ Dharan M (September 2009). "Hyaline globules in ectopic decidua in a pregnant woman with cervical squamous cell carcinoma". Diagn. Cytopathol. 37 (9): 696–8. doi:10.1002/dc.21113. PMID 19526574.
- ↑ 4.0 4.1 4.2 Arias-Stella, J. (Jan 2002). "The Arias-Stella reaction: facts and fancies four decades after.". Adv Anat Pathol 9 (1): 12-23. PMID 11756756.
- ↑ 5.0 5.1 Tadrous, Paul.J. Diagnostic Criteria Handbook in Histopathology: A Surgical Pathology Vade Mecum (1st ed.). Wiley. pp. 236-7. ISBN 978-0470519035.
- ↑ URL: http://pathblog.wordpress.com/2009/01/23/what-is-arias-stella/. Accessed on: September 8, 2014.
- ↑ Doust, J. (Oct 2012). "A is for aphorism - a woman is pregnant until proven otherwise.". Aust Fam Physician 41 (10): 827. PMID 23210111. http://www.racgp.org.au/afp/2012/october/a-is-for-aphorism/.
- ↑ 8.0 8.1 Saxon, D.; Falcone, T.; Mascha, EJ.; Marino, T.; Yao, M.; Tulandi, T. (Jul 1997). "A study of ruptured tubal ectopic pregnancy.". Obstet Gynecol 90 (1): 46-9. doi:10.1016/S0029-7844(97)00180-4. PMID 9207811.