Osteoid osteoma
Jump to navigation
Jump to search
The printable version is no longer supported and may have rendering errors. Please update your browser bookmarks and please use the default browser print function instead.
| Osteoid osteoma | |
|---|---|
| Diagnosis in short | |
 Osteoid osteoma. H&E stain. | |
|
| |
| LM | anastomosing bony trabeculae with variable mineralization, osteoblast rimming, no nuclear atypia of osteocytes |
| LM DDx | osteoblastoma, osteosarcoma |
| Site | bone (femur > tibia > spine > elsewhere) |
|
| |
| Clinical history | pain relieved by NSAIDs |
| Symptoms | extremely painful |
| Radiology | <= 2.0 cm (larger lesions osteoblastoma) |
| Clin. DDx | osteosarcoma |
Osteoid osteoma, abbreviated OO, is benign primary bone tumour. It is grouped with the chondro-osseous tumours.
It should not be confused with an osteoma.
General
- Benign bone lesion.
Clinical:[1]
- Extremely painful.
- Relieved by NSAIDs.
Gross
- Bone: femur > tibia > spine > elsewhere.[2][3]
- Most common location (in bone): diaphysis.[2]
- Must be less than 2 cm - as per WHO definition.[4] ‡
- Larger lesions with the same microscopy are osteoblastomas.
- Central nidus with surround sclerotic bone.[5]
Note:
- ‡ Previously, the diagnostic size cutoff was <=1.5 cm.[6]
Images:
Microscopic
Features:[1]
- Anastomosing bony trabeculae with:
- Variable mineralization.
- Mineralization (calcium phosphate) = purple on H&E stain.
- Osteoblast rimming.
- Cells line-up at edge of bone.
- Variable mineralization.
Note:
- Histomorphologically near identical/indistinguishable from osteoblastoma;[6] one needs some history to make the diagnosis.
DDx:
- Osteosarcoma - lace-like osteoid, no nidus.
- Osteoblastoma - larger lesion, clinical features different.
Images
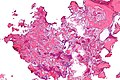
Osteoid osteoma - low mag. (WC)
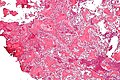
Osteoid osteoma - intermed. mag. (WC)
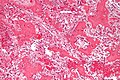
Osteoid osteoma - high mag. (WC)

Osteoid osteoma - very high mag. (WC)



{kind=link}
www:
Sign out
BONE, RIGHT FEMUR, EXCISION: - OSTEOID OSTEOMA.
Micro
The sections show anastomosing bony trabeculae with variable mineralization and osteoblastic rimming. Multinucleated osteoclasts are scattered through the lesion. Hemosiderin-laden macrophages are present. No osteocyte nuclear atypia is apparent. Mitotic activity is not apparent. The osteoid is not lace-like.
See also
References
- ↑ 1.0 1.1 Mills, Stacey E; Carter, Darryl; Greenson, Joel K; Oberman, Harold A; Reuter, Victor E (2004). Sternberg's Diagnostic Surgical Pathology (4th ed.). Lippincott Williams & Wilkins. pp. 285. ISBN 978-0781740517.
- ↑ 2.0 2.1 URL: http://radiology.uthscsa.edu/CME/ELTXT/OOT/skeletallocation.html http://radiology.uthscsa.edu/CME/ELTXT/OOT/skeletallocation.html]. Accessed on: 7 May 2012.
- ↑ URL: http://www.radiologyassistant.nl/en/494e15cbf0d8d. Accessed on: 7 May 2012.
- ↑ Yalcinkaya, U.; Doganavsargil, B.; Sezak, M.; Kececi, B.; Argin, M.; Basdemir, G.; Oztop, F. (Dec 2014). "Clinical and morphological characteristics of osteoid osteoma and osteoblastoma: a retrospective single-center analysis of 204 patients.". Ann Diagn Pathol 18 (6): 319-25. doi:10.1016/j.anndiagpath.2014.08.006. PMID 25224389.
- ↑ Boscainos, PJ.; Cousins, GR.; Kulshreshtha, R.; Oliver, TB.; Papagelopoulos, PJ. (Oct 2013). "Osteoid osteoma.". Orthopedics 36 (10): 792-800. doi:10.3928/01477447-20130920-10. PMID 24093694.
- ↑ 6.0 6.1 Mills, Stacey E; Carter, Darryl; Greenson, Joel K; Oberman, Harold A; Reuter, Victor E (2004). Sternberg's Diagnostic Surgical Pathology (4th ed.). Lippincott Williams & Wilkins. pp. 286. ISBN 978-0781740517.
- ↑ URL: http://njms2.umdnj.edu/tutorweb/gross.htm. Accessed on: 7 May 2012.