Difference between revisions of "Lipoma"
Jump to navigation
Jump to search
(tweak) |
|||
| (9 intermediate revisions by the same user not shown) | |||
| Line 4: | Line 4: | ||
| Width = | | Width = | ||
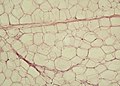
| Caption = Mature adipose tissue (lipoma). [[H&E stain]]. | | Caption = Mature adipose tissue (lipoma). [[H&E stain]]. | ||
| Synonyms = [[steatoma]] (old term, ambiguous) | |||
| Micro = mature adipocytes | | Micro = mature adipocytes | ||
| Subtypes = | | Subtypes = | ||
| Line 10: | Line 11: | ||
| IHC = S-100 +ve | | IHC = S-100 +ve | ||
| EM = | | EM = | ||
| Molecular = | | Molecular = MDM2/CDK4 amplification absent | ||
| IF = | | IF = | ||
| Gross = soft yellow tissue - typically with a thin capsule and lobulated | | Gross = soft yellow tissue - typically with a thin capsule and lobulated | ||
| Line 18: | Line 19: | ||
| Syndromes = | | Syndromes = | ||
| Clinicalhx = | | Clinicalhx = | ||
| Signs = | | Signs = [[pillow sign]] (endoscopy) | ||
| Symptoms = | | Symptoms = | ||
| Prevalence = common | | Prevalence = common | ||
| Bloodwork = | | Bloodwork = | ||
| Rads = | | Rads = | ||
| Endoscopy = | | Endoscopy = smooth yellow coloured submucosal lesion | ||
| Prognosis = benign | | Prognosis = benign | ||
| Other = | | Other = | ||
| ClinDDx = | | ClinDDx = | ||
| Tx = surgical removal or follow-up | |||
}} | }} | ||
'''Lipoma''' is a benign [[adipocytic tumours|adipocytic tumour]]. | '''Lipoma''' is a benign [[adipocytic tumours|adipocytic tumour]]. | ||
| Line 34: | Line 36: | ||
*Several variants exist. | *Several variants exist. | ||
**Angiolipoma - one of the (classically) [[painful skin lesions]]. | **Angiolipoma - one of the (classically) [[painful skin lesions]]. | ||
*May be seen in association with MERRF syndrome (myoclonic epilepsy with ragged-red fibres).<ref name=pmid21865105>{{Cite journal | last1 = Jones | first1 = AP. | last2 = Lewis | first2 = CJ. | last3 = Dildey | first3 = P. | last4 = Hide | first4 = G. | last5 = Ragbir | first5 = M. | title = Lipoma or liposarcoma? A cautionary case report. | journal = J Plast Reconstr Aesthet Surg | volume = 65 | issue = 1 | pages = e11-4 | month = Jan | year = 2012 | doi = 10.1016/j.bjps.2011.08.004 | PMID = 21865105 }}</ref> | |||
*May be seen in the context of ''[[Madelung's disease]]''.<ref name=pmid29129710>{{Cite journal | last1 = Mayo Yáñez | first1 = M. | last2 = González Poggioli | first2 = N. | last3 = Álvarez-Buylla Blanco | first3 = M. | last4 = Herranz González-Botas | first4 = J. | title = Benign symmetric lipomatosis with lingual involvement: Case report and literature review. | journal = J Stomatol Oral Maxillofac Surg | volume = | issue = | pages = | month = Nov | year = 2017 | doi = 10.1016/j.jormas.2017.11.006 | PMID = 29129710 }}</ref> | |||
==Gross== | ==Gross== | ||
| Line 40: | Line 44: | ||
Note: | Note: | ||
*May be quite large ~10 cm. | *May be quite large ~10 cm. | ||
*Thigh lesions are more likely to the malignant than other sites.<ref name=pmid27020493/> | |||
==Microscopic== | ==Microscopic== | ||
| Line 94: | Line 99: | ||
Image:Yellow_adipose_tissue_in_paraffin_section_-_lipids_washed_out.jpg | Mature fat. (WC) | Image:Yellow_adipose_tissue_in_paraffin_section_-_lipids_washed_out.jpg | Mature fat. (WC) | ||
</gallery> | </gallery> | ||
==Molecular== | |||
*MDM2/CDK4 gene amplification absent. | |||
**Testing suggested in lesions greater than 10 cm, thigh lesions and lesions with cytologic atypia.<ref name=pmid27020493>{{Cite journal | last1 = Wong | first1 = DD. | last2 = Low | first2 = IC. | last3 = Peverall | first3 = J. | last4 = Robbins | first4 = PD. | last5 = Spagnolo | first5 = DV. | last6 = Nairn | first6 = R. | last7 = Carey-Smith | first7 = RL. | last8 = Wood | first8 = D. | title = MDM2/CDK4 gene amplification in large/deep-seated 'lipomas': incidence, predictors and clinical significance. | journal = Pathology | volume = 48 | issue = 3 | pages = 203-9 | month = Apr | year = 2016 | doi = 10.1016/j.pathol.2016.02.007 | PMID = 27020493 }}</ref> | |||
==Sign out== | ==Sign out== | ||
===Large lesion looks like lipoma=== | |||
Bland lesions may be well-differentiated liposarcoma.<ref>URL: [https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3422587/ https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3422587/]. Accessed on: 3 June 2017.</ref> Lesions >10 cm should be of concern. | |||
<pre> | |||
Lesion (Submitted as "Lipoma"), Right Neck, Excision: | |||
- Bland appearing adipose tissue suggestive of lipoma, see comment. | |||
- One benign lymph node. | |||
Comment: | |||
Due to the size of the lesion, the case will be sent to a soft tissue pathologist for review. | |||
</pre> | |||
===Block letter=== | |||
<pre> | <pre> | ||
SUBCUTANEOUS TISSUE ("LIPOMA"), LEFT AXILLA, EXCISION: | SUBCUTANEOUS TISSUE ("LIPOMA"), LEFT AXILLA, EXCISION: | ||
Latest revision as of 20:56, 10 December 2018
| Lipoma | |
|---|---|
| Diagnosis in short | |
 Mature adipose tissue (lipoma). H&E stain. | |
|
| |
| Synonyms | steatoma (old term, ambiguous) |
|
| |
| LM | mature adipocytes |
| LM DDx | liposarcoma, benign fat |
| IHC | S-100 +ve |
| Molecular | MDM2/CDK4 amplification absent |
| Gross | soft yellow tissue - typically with a thin capsule and lobulated |
| Site | soft tissue |
|
| |
| Signs | pillow sign (endoscopy) |
| Prevalence | common |
| Endoscopy | smooth yellow coloured submucosal lesion |
| Prognosis | benign |
| Treatment | surgical removal or follow-up |
Lipoma is a benign adipocytic tumour.
General
- Benign.
- Several variants exist.
- Angiolipoma - one of the (classically) painful skin lesions.
- May be seen in association with MERRF syndrome (myoclonic epilepsy with ragged-red fibres).[1]
- May be seen in the context of Madelung's disease.[2]
Gross
- Soft yellow tissue - typically lobulated and with a very thin capsule.
Note:
- May be quite large ~10 cm.
- Thigh lesions are more likely to the malignant than other sites.[3]
Microscopic
Features:
- Collection of mature adipocytes.
- Variation of size may be seen -- should prompt a search for lipoblasts.[4]
Notes:
- Microscopically not definitely distinguishable from mature clump of fat.
- The lesion must be labeled lipoma (by the clinican) to be signed-out as such.
DDx:
- Liposarcoma - increased number of blood vessels,[5] esp. chickenwire-like vessels, fibrous septae.
- Benign adipose tissue.
Images:
Variants
Angiolipoma
Microscopic:
- Numerous blood vessels present.
- +/-Microthrombi.
DDx:
Myolipoma
General:
Microscopic:[8]
- Mature adipose tissue.
- Benign smooth muscle - usually ~ 2x amount of fat.
Note:
- If skeletal muscle is present consider intramuscular lipoma.[10]
IHC:[8]
- Actin +ve.
- Desmin +ve.
Images:
Images

Lipoma - intermed. mag.

Lipoma - high mag.
Mature fat. (WC)


Molecular
- MDM2/CDK4 gene amplification absent.
- Testing suggested in lesions greater than 10 cm, thigh lesions and lesions with cytologic atypia.[3]
Sign out
Large lesion looks like lipoma
Bland lesions may be well-differentiated liposarcoma.[12] Lesions >10 cm should be of concern.
Lesion (Submitted as "Lipoma"), Right Neck, Excision: - Bland appearing adipose tissue suggestive of lipoma, see comment. - One benign lymph node. Comment: Due to the size of the lesion, the case will be sent to a soft tissue pathologist for review.
Block letter
SUBCUTANEOUS TISSUE ("LIPOMA"), LEFT AXILLA, EXCISION:
- MATURE ADIPOSE TISSUE CONSISTENT WITH LIPOMA.
LESION ("LIPOMA"), SPERMATIC CORD (LATERALITY NOT SPECIFIED), EXCISION:
- MATURE ADIPOSE TISSUE CONSISTENT WITH LIPOMA.
Colonic lipoma (clinically suspected)
B. SIGMOID COLON AT 55 CM, BIOPSY: - COLORECTAL-TYPE MUCOSA WITHIN NORMAL LIMITS WITH A SMALL AMOUNT OF SUBMUCOSAL ADIPOSE TISSUE; COMPATIBLE WITH CLINICAL IMPRESSION OF LIPOMA.
Mirco
The sections show mature adipocytes. There is no increase in vascularity. No thick fibrous septa are present.
See also
References
- ↑ Jones, AP.; Lewis, CJ.; Dildey, P.; Hide, G.; Ragbir, M. (Jan 2012). "Lipoma or liposarcoma? A cautionary case report.". J Plast Reconstr Aesthet Surg 65 (1): e11-4. doi:10.1016/j.bjps.2011.08.004. PMID 21865105.
- ↑ Mayo Yáñez, M.; González Poggioli, N.; Álvarez-Buylla Blanco, M.; Herranz González-Botas, J. (Nov 2017). "Benign symmetric lipomatosis with lingual involvement: Case report and literature review.". J Stomatol Oral Maxillofac Surg. doi:10.1016/j.jormas.2017.11.006. PMID 29129710.
- ↑ 3.0 3.1 Wong, DD.; Low, IC.; Peverall, J.; Robbins, PD.; Spagnolo, DV.; Nairn, R.; Carey-Smith, RL.; Wood, D. (Apr 2016). "MDM2/CDK4 gene amplification in large/deep-seated 'lipomas': incidence, predictors and clinical significance.". Pathology 48 (3): 203-9. doi:10.1016/j.pathol.2016.02.007. PMID 27020493.
- ↑ Mentzel, T.; Fletcher, CD. (1995). "Lipomatous tumours of soft tissues: an update.". Virchows Arch 427 (4): 353-63. PMID 8548119.
- ↑ Yang, YJ.; Damron, TA.; Cohen, H.; Hojnowski, L. (Oct 2001). "Distinction of well-differentiated liposarcoma from lipoma in two patients with multiple well-differentiated fatty masses.". Skeletal Radiol 30 (10): 584-9. doi:10.1007/s002560100395. PMID 11685482.
- ↑ Friedberg, MK.; Chang, IL.; Silverman, NH.; Ramamoorthy, C.; Chan, FP. (May 2006). "Images in cardiovascular medicine. Near sudden death from cardiac lipoma in an adolescent.". Circulation 113 (21): e778-9. doi:10.1161/CIRCULATIONAHA.105.589630. PMID 16735681. http://circ.ahajournals.org/content/113/21/e778.full.
- ↑ URL: http://www.webmedcentral.com/article_view/1878. Accessed on: 14 March 2013.
- ↑ 8.0 8.1 8.2 Murphey, MD.; Carroll, JF.; Flemming, DJ.; Pope, TL.; Gannon, FH.; Kransdorf, MJ.. "From the archives of the AFIP: benign musculoskeletal lipomatous lesions.". Radiographics 24 (5): 1433-66. doi:10.1148/rg.245045120. PMID 15371618. http://radiographics.rsna.org/content/24/5/1433.long.
- ↑ Meis, JM.; Enzinger, FM. (Feb 1991). "Myolipoma of soft tissue.". Am J Surg Pathol 15 (2): 121-5. PMID 1703396.
- ↑ URL: http://surgpathcriteria.stanford.edu/softfat/lipoma/intramuscular_lipoma.html. Accessed on: 14 March 2013.
- ↑ Lee, YS.; Park, SE.; Lee, JU.; Choi, ES.. "MRI of a subcutaneous myolipoma in the ankle: a case report.". Korean J Radiol 12 (5): 641-5. doi:10.3348/kjr.2011.12.5.641. PMC 3168809. PMID 21927569. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3168809/.
- ↑ URL: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3422587/. Accessed on: 3 June 2017.