Difference between revisions of "Keratoacanthoma"
(+gross) |
(→Sign out: +nonbelivers of KA) |
||
| (7 intermediate revisions by 2 users not shown) | |||
| Line 1: | Line 1: | ||
{{ Infobox diagnosis | |||
| Name = {{PAGENAME}} | |||
| Image = Skin_keratoacanthoma_whole_slide.jpg | |||
| Width = | |||
| Caption = Keratoacanthoma. [[H&E stain]]. | |||
| Micro = keratin plug, downward cupping of the epidermis, minimal keratinocyte atypia, +/- keratinocytes with glassy pink cytoplasm | |||
| Subtypes = | |||
| LMDDx = [[squamous cell carcinoma of the skin|squamous cell carcinoma]], [[verruca vulgaris]], [[pseudoepitheliomatous hyperplasia]] | |||
| Stains = | |||
| IHC = | |||
| EM = | |||
| Molecular = | |||
| IF = | |||
| Gross = | |||
| Grossing = | |||
| Site = | |||
| Assdx = | |||
| Syndromes = | |||
| Clinicalhx = | |||
| Signs = rapid growth | |||
| Symptoms = | |||
| Prevalence = uncommon | |||
| Bloodwork = | |||
| Rads = | |||
| Endoscopy = | |||
| Prognosis = good | |||
| Other = | |||
| ClinDDx = [[squamous cell carcinoma of the skin|squamous cell carcinoma]] | |||
}} | |||
'''Keratoacanthoma''' is clinically worrisome lesion that classically arise on the nose. | '''Keratoacanthoma''' is clinically worrisome lesion that classically arise on the nose. | ||
It is abbreviated '''KA'''. | It is abbreviated '''KA'''. | ||
| Line 12: | Line 41: | ||
==Gross== | ==Gross== | ||
*Raised dome-like lesions with a central defect. | *Raised dome-like lesions with a central crater-like defect. | ||
<gallery> | <gallery> | ||
Image:Keratoacanthoma_2.jpg | Keratoacanthoma. (WC) | Image:Keratoacanthoma_2.jpg | Keratoacanthoma. (WC) | ||
</gallery> | </gallery> | ||
==Microscopic== | ==Microscopic== | ||
Features:<ref name=Ref_Klatt378>{{Ref Klatt|378}}</ref> | Features:<ref name=Ref_Klatt378>{{Ref Klatt|378}}</ref> | ||
| Line 36: | Line 66: | ||
<gallery> | <gallery> | ||
Image:Skin_keratoacanthoma_whole_slide.jpg | Keratoacanthoma. (WC) | Image:Skin_keratoacanthoma_whole_slide.jpg | Keratoacanthoma. (WC) | ||
Image:Keratoacanthoma_(1),_H%26E.jpg | Keratoacanthoma. (WC/euthman) | |||
Image:Keratoacanthoma (2), H&E.jpg | Keratoacanthoma. (WC/euthman) | |||
Image:Keratoacanthoma (3), H&E.jpg | Keratoacanthoma. (WC/euthman) | |||
</gallery> | </gallery> | ||
==Sign out== | |||
<pre> | |||
LESION, LEFT SIDE OF NOSE, EXCISION: | |||
- KERATOACANTHOMA. | |||
- SOLAR ELASTOSIS. | |||
</pre> | |||
====Micro==== | |||
The sections show hair-bearing skin with a dome-shaped lesion that consists of a cup-shaped epidermal rim, and a large plug of keratin. The lesion is surrounded by a mild patchy lymphoplasmacytic infiltrate. No mitotic activity is apparent. The keratinocytes have minimal atypia and mature to the surface. A granular layer is present. The lesion is completely excised in the plane of section. | |||
There is no hypergranulosis. No koilocytes are seen. Solar elastosis is present. | |||
===Non-believers in the diagnosis=== | |||
<pre> | |||
Skin Lesion, Left Leg, Excision: | |||
- WELL-DIFFERENTIATED SQUAMOUS CELL CARCINOMA, KERATOACANTHOMA-LIKE, | |||
margins clear. | |||
</pre> | |||
====Micro==== | |||
The sections show hair-bearing skin with a dome-shaped lesion that consists of a cup-shaped epidermal rim, and a large plug of keratin. The lesion has a pushing border and is surrounded by a mild patchy lymphoplasmacytic infiltrate. Mitotic activity is not readily apparent. The keratinocytes have minimal atypia. The lesion is completely excised in the plane of section. No koilocytes are seen. Solar elastosis is present. | |||
==See also== | ==See also== | ||
Latest revision as of 18:18, 21 December 2020
| Keratoacanthoma | |
|---|---|
| Diagnosis in short | |
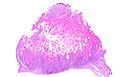
 Keratoacanthoma. H&E stain. | |
|
| |
| LM | keratin plug, downward cupping of the epidermis, minimal keratinocyte atypia, +/- keratinocytes with glassy pink cytoplasm |
| LM DDx | squamous cell carcinoma, verruca vulgaris, pseudoepitheliomatous hyperplasia |
| Signs | rapid growth |
| Prevalence | uncommon |
| Prognosis | good |
| Clin. DDx | squamous cell carcinoma |
Keratoacanthoma is clinically worrisome lesion that classically arise on the nose. It is abbreviated KA.
General
- Generally considered to be benign.
- Rare reports of metastases suggesting it may be a form of squamous cell carcinoma.[1]
Clinical
- May grow rapidly (weeks or months) then involute.
- Main DDx is squamous cell carcinoma.
- Exophytic lesion, well-circumscribed.
Gross
- Raised dome-like lesions with a central crater-like defect.

Keratoacanthoma. (WC)

Microscopic
Features:[2]
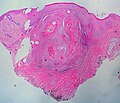
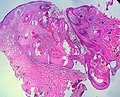
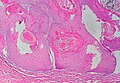
- Expansion of stratum spinosum - pushing tongue-like downward growth of epidermis into the dermis.
- Keratin collection ("keratin plug") at the center of lesion-superficial aspect.
- Cells have glassy pink cytoplasm.
- Minimal/no nuclear atypia.
Note:
- Classically described as a "volcano lesion" with pale pink cells.
- May have features of regression - PMNs, fibrosis (???).
DDx:[3]
- Verruca vulgaris.
- Conventional squamous cell carcinoma of the skin with a cup-shape.
- Pseudoepitheliomatous hyperplasia.
Image
Keratoacanthoma. (WC)
Keratoacanthoma. (WC/euthman)
Keratoacanthoma. (WC/euthman)
Keratoacanthoma. (WC/euthman)
,_H%26E.jpg)
,_H%26E.jpg)
,_H%26E.jpg)
Sign out
LESION, LEFT SIDE OF NOSE, EXCISION: - KERATOACANTHOMA. - SOLAR ELASTOSIS.
Micro
The sections show hair-bearing skin with a dome-shaped lesion that consists of a cup-shaped epidermal rim, and a large plug of keratin. The lesion is surrounded by a mild patchy lymphoplasmacytic infiltrate. No mitotic activity is apparent. The keratinocytes have minimal atypia and mature to the surface. A granular layer is present. The lesion is completely excised in the plane of section.
There is no hypergranulosis. No koilocytes are seen. Solar elastosis is present.
Non-believers in the diagnosis
Skin Lesion, Left Leg, Excision:
- WELL-DIFFERENTIATED SQUAMOUS CELL CARCINOMA, KERATOACANTHOMA-LIKE,
margins clear.
Micro
The sections show hair-bearing skin with a dome-shaped lesion that consists of a cup-shaped epidermal rim, and a large plug of keratin. The lesion has a pushing border and is surrounded by a mild patchy lymphoplasmacytic infiltrate. Mitotic activity is not readily apparent. The keratinocytes have minimal atypia. The lesion is completely excised in the plane of section. No koilocytes are seen. Solar elastosis is present.
See also
References
- ↑ Mandrell JC, Santa Cruz D (August 2009). "Keratoacanthoma: hyperplasia, benign neoplasm, or a type of squamous cell carcinoma?". Semin Diagn Pathol 26 (3): 150–63. PMID 20043514.
- ↑ Klatt, Edward C. (2006). Robbins and Cotran Atlas of Pathology (1st ed.). Saunders. pp. 378. ISBN 978-1416002741.
- ↑ Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 379. ISBN 978-0443066542.