Helicobacter gastritis
| Helicobacter gastritis | |
|---|---|
| Diagnosis in short | |
 Helicobacter gastritis. H&E stain. | |
|
| |
| LM | helicobacter organisms, moderate chronic active gastritis (neutrophils esp. at the luminal aspect/intraepithelial, numerous plasma cell clusters) |
| Subtypes | Helicobacter pylori, Helicobacter heilmannii |
| LM DDx | acute gastritis, chronic gastritis |
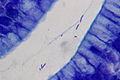
| Stains | Diff-Quik, Cresyl violet stain, Warthin-Starry stain |
| IHC | Helicobacter IHC |
| Site | stomach |
|
| |
| Associated Dx | MALT lymphoma, gastric carcinoma, intestinal metaplasia of the stomach, peptic ulcer, duodenitis |
| Prevalence | common |
| Endoscopy | erythema |
| Prognosis | benign |
| Clin. DDx | normal stomach |
Helicobacter gastritis, abbreviated HG, is a common form of gastritis caused by Helicobacter species.
The most common Helicobacter implicated is Helicobacter pylori, abbreviated HP.
General
- Several Helicobacter species can cause gastritis:
- Helicobacter pylori - most common.
- Helicobacter heilmannii.
Epidemiologic associations - Helicobacter infections are associated with:[1]
- Gastritis.
- Peptic ulcers.
- Cancer.
- Carcinoma.
- MALT lymphoma.
Note:
- Historically, Helicobacter was grouped with Campylobacter.[2]
- This is why it is the rapid urease test, sometimes done at endoscopy, is also known as the Campylobacter-like organism test, abbreviated CLO test.
Gross
- Thickened gastric folds.
- Erythema.
Microscopic
Features:
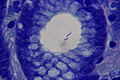
- Helicobacter organisms - key feature.
- Inflammation - usually moderate chronic active.
- Clusters of (lamina propria) plasma cells.
- Neutrophils, numerous, classically intraepithelial and superficial.
Tips:
- One needs to look at 400x magnification. Even at 400x they are possible to miss.
- Helicobacter are damn small. They are smaller than the nucleus of the gastric foveollar cell.
- Look for mucus - they preferentially reside there.
- This is usually close to the opening of the gastric pits.
- Helicobacter are found in groups. When you see several that are the same size and shape you can be sure they are real.
Notes:
- Helicobacter can be in antrum and/or body.[5]
- Helicobacter don't like the intestinal mucosa or mucosa that has undergone intestinal metaplasia; you're less likely to find 'em adjacent to it. In general, Helicobacter is uncommon in the context of a case with IM... but common enough that one still ought to look for it.
- May be associated with G-cell hyperplasia.[6]
DDx:
- Dirt - material has a variable size.
- Contamination from oropharynx - bacilli straight, not associated with gastric mucosa.
- Chronic gastritis.
- Acute gastritis.
Images
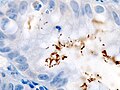
H. pylori - IHC. (WC)
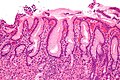
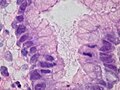
Gastritis due to HP. (WC)
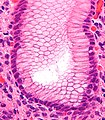
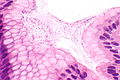
HP visible. (WC)
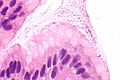
HP gastritis. (WC)
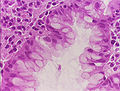
HP gastritis. (WC)
HP gastritis. (WC)





.jpg)

HP - very high mag. (WC)
HP - extremely high mag. (WC)
HP - extremely high mag. (WC)

HP - extremely high mag. (WC)



www:
Helicobacter heilmannii
HH. (WC/Patho)

HH. (WC/Patho)
HH. (WC/Patho)



{kind=link}
Stains
- Cresyl violet stain - background and organisms blue.
- Warthin-Starry stain - background yellow, organisms black.
IHC
- Helicobacter pylori IHC stain +ve.
Note:
- Reportly also stains Helicobacter heilmannii.[4]
Sign out
Body
Stomach, Biopsy: - Body-type gastric mucosa with moderate chronic active inflammation and abundant HELICOBACTER-LIKE ORGANISMS. - NEGATIVE for intestinal metaplasia. - NEGATIVE for dysplasia and NEGATIVE for malignancy.
IELs in duodenum
A. Duodenum, Biopsy: - Small bowel mucosa with increased intraepithelial lymphocytes, villous architecture and crypt architecture within normal limits, see comment. - NEGATIVE for acute duodenitis. - NEGATIVE for dysplasia. B. Stomach, Biopsy: - Body-type gastric mucosa with moderate chronic active inflammation and abundant HELICOBACTER-LIKE ORGANISMS. - NEGATIVE for intestinal metaplasia. - NEGATIVE for dysplasia and NEGATIVE for malignancy. COMMENT: There are approximately 45 lymphocytes/100 enterocytes. Increased intraepithelial lymphocytes (IELs) is a nonspecific finding. IELs are seen in celiac disease and inflammatory bowel disease; however, may be explained by the Helicobacter-like organisms found in the stomach. Clinical correlation is suggested.
Alternate comment
Comment: Focally, there are approximately 50 lymphocytes/100 enterocytes. Increased intraepithelial lymphocytes is a nonspecific finding that may be seen in a number of conditions, including infections (e.g. Helicobacter gastritis), and autoimmune disorders (e.g. Crohn's disease, celiac disease). In this case, it may be explained by the Helicobacter-like organisms found in the stomach. Clinical correlation is suggested.
Block letters
STOMACH, BIOPSY: - BODY-TYPE GASTRIC MUCOSA WITH MODERATE CHRONIC ACTIVE INFLAMMATION. - ABUNDANT HELICOBACTER-LIKE ORGANISMS PRESENT. - NEGATIVE FOR INTESTINAL METAPLASIA. - NEGATIVE FOR DYSPLASIA AND NEGATIVE FOR MALIGNANCY.
Antrum
Stomach, Biopsy: - Antral-type gastric mucosa with moderate chronic active inflammation. - Abundant Helicobacter-like organisms present. - NEGATIVE for intestinal metaplasia. - NEGATIVE for dysplasia and NEGATIVE for malignancy.
Block letters
STOMACH, BIOPSY: - ANTRAL-TYPE GASTRIC MUCOSA WITH MODERATE CHRONIC ACTIVE INFLAMMATION. - ABUNDANT HELICOBACTER-LIKE ORGANISMS PRESENT. - NEGATIVE FOR INTESTINAL METAPLASIA. - NEGATIVE FOR DYSPLASIA AND NEGATIVE FOR MALIGNANCY.
IM present
Stomach, Biopsy: - Antral-type gastric mucosa with: -- Focal intestinal metaplasia. -- Abundant Helicobacter-like organisms. -- Moderate chronic active gastritis. - NEGATIVE for dysplasia and NEGATIVE for malignancy.
Block letters
STOMACH, BIOPSY: - ANTRAL-TYPE GASTRIC MUCOSA WITH: -- FOCAL INTESTINAL METAPLASIA. -- ABUNDANT HELICOBACTER-LIKE ORGANISMS. -- MODERATE CHRONIC ACTIVE INFLAMMATION. - NEGATIVE FOR DYSPLASIA AND NEGATIVE FOR MALIGNANCY.
H. heilmannii
Stomach, Biopsy: - Antral-type gastric mucosa with moderate chronic active inflammation. - Abundant Helicobacter-like organisms present. - NEGATIVE for intestinal metaplasia. - NEGATIVE for dysplasia and NEGATIVE for malignancy. Comment: The Helicobacter-like organisms have an appearance similar to crinkle cut French fries; this suggests the organisms are H. heilmannii.
Micro
The sections show antral-type gastric mucosa with abundant lamina propria plasma cells and focal intraepithelial neutrophils. Cocci and bacilli are present. Some of the bacilli are Helicobactor-like. The epithelium matures normally to the surface. No goblet cells are identified.
See also
References
- ↑ Cotran, Ramzi S.; Kumar, Vinay; Fausto, Nelson; Nelso Fausto; Robbins, Stanley L.; Abbas, Abul K. (2005). Robbins and Cotran pathologic basis of disease (7th ed.). St. Louis, Mo: Elsevier Saunders. pp. 814. ISBN 0-7216-0187-1.
- ↑ Ciortescu, I.; Stan, M.. "[Helicobacter pylori--friend or foe?].". Rev Med Chir Soc Med Nat Iasi 114 (3): 619-24. PMID 21243784.
- ↑ Mobley, HLT.; Mendz, GL.; Hazell, SL.; Andersen, LP.; Wadström, T.. Basic Bacteriology and Culture. PMID 21290743. http://www.ncbi.nlm.nih.gov/books/NBK2444/.
- ↑ 4.0 4.1 Singhal, AV.; Sepulveda, AR. (Nov 2005). "Helicobacter heilmannii gastritis: a case study with review of literature.". Am J Surg Pathol 29 (11): 1537-9. PMID 16224223.
- ↑ Maaroos HI, Kekki M, Villako K, Sipponen P, Tamm A, Sadeniemi L (October 1990). "The occurrence and extent of Helicobacter pylori colonization and antral and body gastritis profiles in an Estonian population sample". Scand. J. Gastroenterol. 25 (10): 1010-7. PMID 2263873.
- ↑ Kwan, CP.; Tytgat, GN. (Nov 1995). "Antral G-cell hyperplasia: a vanishing disease?". Eur J Gastroenterol Hepatol 7 (11): 1099-1103. PMID 8680911.
- ↑ URL: http://gut.bmj.com/content/58/12/1669.extract. Accessed on: 2 March 2012.