Difference between revisions of "Follicular lymphoma"
Jump to navigation
Jump to search
m (→IHC) |
m |
||
| Line 5: | Line 5: | ||
| Caption = | | Caption = | ||
| Synonyms = | | Synonyms = | ||
| Micro = Lymph node | | Micro = Lymph node: abundant abnormally-shaped lymphoid follicles with some of the following: non-polarized mantle zone, non-polarized germinal center, loss of tingible body macrophages, sinuses effaced (lost) | ||
| Subtypes = | | Subtypes = | ||
| LMDDx = [[diffuse large B-cell lymphoma]], other [[small cell lymphomas]], reactive follicular hyperplasia | | LMDDx = [[diffuse large B-cell lymphoma]], other [[small cell lymphomas]], reactive follicular hyperplasia | ||
Revision as of 02:07, 30 December 2013
| Follicular lymphoma | |
|---|---|
| Diagnosis in short | |
.jpg) | |
|
| |
| LM | Lymph node: abundant abnormally-shaped lymphoid follicles with some of the following: non-polarized mantle zone, non-polarized germinal center, loss of tingible body macrophages, sinuses effaced (lost) |
| LM DDx | diffuse large B-cell lymphoma, other small cell lymphomas, reactive follicular hyperplasia |
| IHC | CD20 +ve, CD10 +ve, BCL-6 +ve, BCL-2 +ve |
| Gross | white lesions +/-subtle fine nodularity (fish flesh-like appearance) |
| Site | lymph node, spleen, bone marrow, others |
|
| |
| Prevalence | common |
| Prognosis | moderate to good |
| Clin. DDx | other causes of lymphadenopathy - other lymphomas, metastatic carcinoma |
Follicular lymphoma, abbreviated FL, is a very common non-Hodgkin lymphoma. It is a small cell lymphoma.
General
- A very common type of lymphoma.
- Moderate prognosis - overall five year survival ~ 66% in one cohort without transformation.[1]
- May transform to a more aggressive lymphoma, e.g. diffuse large B-cell lymphoma.
Gross
- Lymph node enlargement.
- Classically white and uniform - usually described as fish flesh-like.
- May have a vague nodularity.
Images

FL in a lymph node. (WC)

FL in the spleen. (WC)


Microscopic
Features (lymph node):
- Abundant abnormally-shaped lymphoid follicles - key feature - including some of the following:
- Non-polarized mantle zone (normal mantle zone is usu. thicker at capsular aspect).
- Non-polarized germinal center (normal germinal center has dark & light area).
- Loss of tingible body macrophages.
- Sinuses effaced (lost).
Note:
- The intrafollicular component of the lymph node is compressed - follicles are often described as "kissing", as they nearly touch.
- In bone marrow specimens the neoplastic cells classically have a paratrabecular arrangement,[2] i.e. the lymphoma cells are found adjacent to the bone spicules.
DDx:
- Reactive follicular hyperplasia.
- Diffuse large B-cell lymphoma - esp. for the grade 3B.
Images
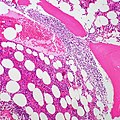
FL - bone marrow. (WC/euthman)
www:
Grading
- Grade 1-2: <= 22 centroblasts / HPF; where 1 HPF ~= 0.2376 mm^2 (22 mm eye piece @ 40X objective).
- Grade 3A: >22 centroblasts / HPF; where 1 HPF ~= 0.2376 mm^2 (22 mm eye piece @ 40X objective).
- Grade 3B: only centroblasts (within a nodular architecture).
Notes:
- Significant interobserver variability.[3]
- Grade 1 & Grade 2 lumped together.
- One should evaluate 10 HPFs.
- Only centroblasts without a nodular architecture is Diffuse large B cell lymphoma (DLBCL).
The usual cut points mentioned by people with HPFitis are:[4]
- Grade 1: 0-5 centroblasts / HPF.
- Grade 2: 5-15 centroblasts / HPF.
- Grade 3: >15 centroblasts / HPF.
IHC
Features:[5]
- CD10 +ve.
- BCL6 +ve.
Others:
- CD5 -ve.
- +ve in mantle cell lymphoma.
- CD23 -ve/+ve.
- +ve in CLL.
- CD43 -ve.
- +ve in mantle cell lymphoma, marginal zone lymphoma.
- CD11c -ve -- flow cytometry only.
- CD21 -ve in tumour cells; highlights follicular dendritic cells.
- BCL2 +ve[5] - like many other small cell lymphomas.
- Usually negative in benign germinal centres.
Image:
{kind=link}
A panel to work-up:
- BCL2, BCL6, CD3, CD5, CD10, CD20, CD23, cyclin D1.
Molecular
- t(14;18)(q32;q21)/IGH-BCL2 in 70-95% of cases.[5]
- Should not be confused with t(14;18)(q32;q21)/IGH-MALT1 seen in MALT lymphomas.[6]
Sign out
RETROPERITONEAL MASS, RIGHT, CORE BIOPSIES: - NON-HODGKIN B-CELL LYMPHOMA, FAVOUR FOLLICULAR LYMPHOMA. COMMENT: Morphology: -Small cells: size ~ mature lymphocytes, quantity - many, angular and round. -Large cells (intermixed with small cells): size ~1.5-2x mature lymphocyte, small nucleoli, moderate quantity of grey/basophilic cytoplasm, moderate nuclear pleomorphism. -Architecture: no gland formation, discohesive, no follicles apparent, no sheets of large cells. -Mitoses are uncommon. Immunohistochemical stains (tumour cells): Positive: CD45 (strong, membranous/cytoplasmic), CD20 (strong, membranous/cytoplasmic), BCL-2 (strong, membranous/cytoplasmic), CD10 (strong, membranous), BCL-6 (moderate, patchy, nuclear). Negative: pankeratin, CD3, CD5, CD30, CD21 (follicular dendritic cells not apparent), CD23 (scattered, rare). Ki-67: highlights the large cells, primarily -- 5-35% of cells within the core. The findings favour a follicular lymphoma, based on the cellular morphology and immunostains; however, they are limited by the type of tissue sampling (core biopsy). Clinical correlation is suggested.
See also
References
- ↑ 1.0 1.1 1.2 Link, BK.; Maurer, MJ.; Nowakowski, GS.; Ansell, SM.; Macon, WR.; Syrbu, SI.; Slager, SL.; Thompson, CA. et al. (Sep 2013). "Rates and outcomes of follicular lymphoma transformation in the immunochemotherapy era: a report from the University of Iowa/MayoClinic Specialized Program of Research Excellence Molecular Epidemiology Resource.". J Clin Oncol 31 (26): 3272-8. doi:10.1200/JCO.2012.48.3990. PMID 23897955.
- ↑ Iancu, D.; Hao, S.; Lin, P.; Anderson, SK.; Jorgensen, JL.; McLaughlin, P.; Medeiros, LJ. (Feb 2007). "Follicular lymphoma in staging bone marrow specimens: correlation of histologic findings with the results of flow cytometry immunophenotypic analysis.". Arch Pathol Lab Med 131 (2): 282-7. doi:10.1043/1543-2165(2007)131[282:FLISBM]2.0.CO;2. PMID 17284114.
- ↑ Good, D. 17 August 2010.
- ↑ Mills, Stacey E; Carter, Darryl; Greenson, Joel K; Oberman, Harold A; Reuter, Victor E (2004). Sternberg's Diagnostic Surgical Pathology (4th ed.). Lippincott Williams & Wilkins. pp. 813. ISBN 978-0781740517.
- ↑ 5.0 5.1 5.2 Vitolo U, Ferreri AJ, Montoto S (June 2008). "Follicular lymphomas". Crit. Rev. Oncol. Hematol. 66 (3): 248–61. doi:10.1016/j.critrevonc.2008.01.014. PMID 18359244.
- ↑ Bacon CM, Du MQ, Dogan A (April 2007). "Mucosa-associated lymphoid tissue (MALT) lymphoma: a practical guide for pathologists". J. Clin. Pathol. 60 (4): 361–72. doi:10.1136/jcp.2005.031146. PMC 2001121. PMID 16950858. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2001121/.