Difference between revisions of "Epilepsy"
Jump to navigation
Jump to search
m (more) |
Jensflorian (talk | contribs) (→Types: MOGHE) |
||
| (12 intermediate revisions by 2 users not shown) | |||
| Line 1: | Line 1: | ||
'''Epilepsy''' is a common chronic seizure disorder. | '''Epilepsy''' is a common chronic seizure disorder. | ||
==Etiology== | ==General== | ||
*Epilepsy = seizures that are "idiopathic", i.e. no brain tumour, no mass lesion, no brain injury. | |||
*Most common form: ''temporal lobe epilepsy''.<ref>URL: [http://emedicine.medscape.com/article/342150-overview http://emedicine.medscape.com/article/342150-overview]. Accessed on: 20 November 2010.</ref> | |||
===Etiology=== | |||
*Many. | *Many. | ||
**[[Epilepsy#Focal_cortical_dysplasia_.28FCD.29|Cortical dysplasia]]. | |||
**[[Epilepsy#Hamartia|Hamartia]]. | |||
**Stroke. | |||
**Infection. | |||
**Head trauma. | |||
Syndromic: | Syndromic: | ||
| Line 10: | Line 19: | ||
*[[Dysembryoplastic neuroepithelial tumour]].<ref name=pmid15881751>{{Cite journal | last1 = Cataltepe | first1 = O. | last2 = Turanli | first2 = G. | last3 = Yalnizoglu | first3 = D. | last4 = Topçu | first4 = M. | last5 = Akalan | first5 = N. | title = Surgical management of temporal lobe tumor-related epilepsy in children. | journal = J Neurosurg | volume = 102 | issue = 3 Suppl | pages = 280-7 | month = Apr | year = 2005 | doi = 10.3171/ped.2005.102.3.0280 | PMID = 15881751 }}</ref> | *[[Dysembryoplastic neuroepithelial tumour]].<ref name=pmid15881751>{{Cite journal | last1 = Cataltepe | first1 = O. | last2 = Turanli | first2 = G. | last3 = Yalnizoglu | first3 = D. | last4 = Topçu | first4 = M. | last5 = Akalan | first5 = N. | title = Surgical management of temporal lobe tumor-related epilepsy in children. | journal = J Neurosurg | volume = 102 | issue = 3 Suppl | pages = 280-7 | month = Apr | year = 2005 | doi = 10.3171/ped.2005.102.3.0280 | PMID = 15881751 }}</ref> | ||
*[[Ganglioglioma]].<ref name=pmid12125968>{{Cite journal | last1 = Im | first1 = SH. | last2 = Chung | first2 = CK. | last3 = Cho | first3 = BK. | last4 = Lee | first4 = SK. | title = Supratentorial ganglioglioma and epilepsy: postoperative seizure outcome. | journal = J Neurooncol | volume = 57 | issue = 1 | pages = 59-66 | month = Mar | year = 2002 | doi = | PMID = 12125968 }}</ref> | *[[Ganglioglioma]].<ref name=pmid12125968>{{Cite journal | last1 = Im | first1 = SH. | last2 = Chung | first2 = CK. | last3 = Cho | first3 = BK. | last4 = Lee | first4 = SK. | title = Supratentorial ganglioglioma and epilepsy: postoperative seizure outcome. | journal = J Neurooncol | volume = 57 | issue = 1 | pages = 59-66 | month = Mar | year = 2002 | doi = | PMID = 12125968 }}</ref> | ||
*Isomorphic astrocytoma. | |||
==Types== | |||
Features:<ref>MUN. 15 November 2010.</ref> | |||
*Temporal lobe epilepsy | |||
*Mesial temporal sclerosis = scarring of the medial temporal lobe. | |||
**Involves: hippocampus, parahippocampal gyrus and amygdala. | |||
*Granule cell dispersion | |||
===Hamartia=== | |||
* Small collection of ectopic glioneuronal cells. | |||
**Morpholology resembling oligodendroglial-like cells. <ref>{{Cite journal | last1 = Kasper | first1 = BS. | last2 = Stefan | first2 = H. | last3 = Buchfelder | first3 = M. | last4 = Paulus | first4 = W. | title = Temporal lobe microdysgenesis in epilepsy versus control brains. | journal = J Neuropathol Exp Neurol | volume = 58 | issue = 1 | pages = 22-8 | month = Jan | year = 1999 | doi = | PMID = 10068310 }}</ref> | |||
* Mostly amygdala, less common in hippocampus or temporal lobe. | |||
* Can coexist with focal cortical dysplasia. | |||
===Focal cortical dysplasia (FCD)=== | |||
*Localized malformations of the cortex. | |||
*Frequently associated with epilepsy in children. | |||
*Includes cortical dyslamination, cytoarchitectural changes and white matter abnormalities. | |||
*Current consensus: ILAE classification scheme 2011 <ref>{{Cite journal | last1 = Blümcke | first1 = I. | last2 = Aronica | first2 = E. | last3 = Miyata | first3 = H. | last4 = Sarnat | first4 = HB. | last5 = Thom | first5 = M. | last6 = Roessler | first6 = K. | last7 = Rydenhag | first7 = B. | last8 = Jehi | first8 = L. | last9 = Krsek | first9 = P. | title = International recommendation for a comprehensive neuropathologic workup of epilepsy surgery brain tissue: A consensus Task Force report from the ILAE Commission on Diagnostic Methods. | journal = Epilepsia | volume = 57 | issue = 3 | pages = 348-58 | month = Mar | year = 2016 | doi = 10.1111/epi.13319 | PMID = 26839983 }} | |||
</ref>(based on previous classification by Palmini 2004): | |||
*Type I FCD (focal) | |||
**Ia: Abnormal radial cortical lamination. | |||
**Ib: Abnormal tangential cortical lamination. | |||
**Ic: Abnormal radial and tangential cortical lamination. | |||
*Type II FCD (focal) | |||
**IIa: Presence of dysmorphic neurons. | |||
**IIb: Presence of dysmorphic neurons and balloon cells. | |||
*Type III FCD (associated with other lesion) | |||
**IIIa: FCD associated with [[Epilepsy#Hippocampal_sclerosis|hippocampal sclerosis]]. | |||
**IIIb: FCD adjacent to a brain tumor. | |||
**IIIc: FCD adjacent to vascular malformation. | |||
**IIIc: FCD associated with previous injury (trauma, inflammation...). | |||
<gallery> | |||
File:FCDIIa dysmorphic neurons HE.jpg|Dysmorphic neurons in FCD (HE) | |||
File:FCDIIa neuronal heterotopia neun.jpg|Heterotopic neurons (NeuN) | |||
</gallery> | |||
===Hippocampal sclerosis=== | |||
*Most frequent histopathology in temporal lobe epilepsy (33% of all epilepsy surgery specimen). | |||
*ILAE classification for hippocampus specimen:<ref>{{Cite journal | last1 = Blümcke | first1 = I. | last2 = Thom | first2 = M. | last3 = Aronica | first3 = E. | last4 = Armstrong | first4 = DD. | last5 = Bartolomei | first5 = F. | last6 = Bernasconi | first6 = A. | last7 = Bernasconi | first7 = N. | last8 = Bien | first8 = CG. | last9 = Cendes | first9 = F. | title = International consensus classification of hippocampal sclerosis in temporal lobe epilepsy: a Task Force report from the ILAE Commission on Diagnostic Methods. | journal = Epilepsia | volume = 54 | issue = 7 | pages = 1315-29 | month = Jul | year = 2013 | doi = 10.1111/epi.12220 | PMID = 23692496 }}</ref> | |||
** ILAE type 1: cell loss predominantly in CA1 and CA4 sectors. | |||
** ILAE type 2: predominant CA1 neuron loss and gliosis. | |||
** ILAE type 3: CA4 predominant neuronal cell loss and gliosis. | |||
Clinic: | |||
ILAE type 1: benefit from epilepsy surgery. | |||
Notes: | |||
*Gliosis withot neuronal loss is not considered hippocampal sclerosis. | |||
===Granule cell dispersion=== | |||
*Affects dentate gyrus. | |||
*Observed in up to 40% specimen with hippocampal sclerosis. | |||
*Clinico-pathological classification:<ref>{{Cite journal | last1 = Blümcke | first1 = I. | last2 = Kistner | first2 = I. | last3 = Clusmann | first3 = H. | last4 = Schramm | first4 = J. | last5 = Becker | first5 = AJ. | last6 = Elger | first6 = CE. | last7 = Bien | first7 = CG. | last8 = Merschhemke | first8 = M. | last9 = Meencke | first9 = HJ. | title = Towards a clinico-pathological classification of granule cell dispersion in human mesial temporal lobe epilepsies. | journal = Acta Neuropathol | volume = 117 | issue = 5 | pages = 535-44 | month = May | year = 2009 | doi = 10.1007/s00401-009-0512-5 | PMID = 19277686 }}</ref> | |||
**Granule cell pathology (GCP) Type 1: Substantial granule cell loss. | |||
**Granule cell pathology (GCP) Type 2: Cell dispersion, ectopic neurons or clusters of neurons in the molecular layer or bi-lamination. | |||
Clinic: | |||
*Association with longer epilepsy duration. | |||
DDx: | |||
**Epilepsy. | |||
**[[Dementia]]. | |||
===Mild Malformation of Cortical Development with Oligodendroglial Hyperplasia=== | |||
* Abbreviated: MOGHE <ref>{{Cite journal | last1 = Schurr | first1 = J. | last2 = Coras | first2 = R. | last3 = Rössler | first3 = K. | last4 = Pieper | first4 = T. | last5 = Kudernatsch | first5 = M. | last6 = Holthausen | first6 = H. | last7 = Winkler | first7 = P. | last8 = Woermann | first8 = F. | last9 = Bien | first9 = CG. | title = Mild Malformation of Cortical Development with Oligodendroglial Hyperplasia in Frontal Lobe Epilepsy: A New Clinico-Pathological Entity. | journal = Brain Pathol | volume = 27 | issue = 1 | pages = 26-35 | month = 01 | year = 2017 | doi = 10.1111/bpa.12347 | PMID = 26748554 }}</ref>. | |||
* Frontal lobe. | |||
* Nonlesional (3.7% of epilepsy case). | |||
* Increase cellularity of Olig2-, and PDGFR-alpha-immunoreactive oligodendroglia. | |||
==Sudden unexpected death in epilepsy== | |||
*Abbreviated ''SUDEP''. | |||
Diagnosis: | |||
*[[Negative autopsy]]. | |||
*History of epilepsy. | |||
Epidemiology:<ref name=pmid18805738>{{Cite journal | last1 = Tomson | first1 = T. | last2 = Nashef | first2 = L. | last3 = Ryvlin | first3 = P. | title = Sudden unexpected death in epilepsy: current knowledge and future directions. | journal = Lancet Neurol | volume = 7 | issue = 11 | pages = 1021-31 | month = Nov | year = 2008 | doi = 10.1016/S1474-4422(08)70202-3 | PMID = 18805738 }}</ref> | |||
*Typically poorly controlled epilepsy. | |||
*Incidence: 0.09-9 per 1000 patient-years. | |||
==See also== | ==See also== | ||
*[[Neuropathology]]. | *[[Neuropathology]]. | ||
Latest revision as of 14:05, 25 March 2019
Epilepsy is a common chronic seizure disorder.
General
- Epilepsy = seizures that are "idiopathic", i.e. no brain tumour, no mass lesion, no brain injury.
- Most common form: temporal lobe epilepsy.[1]
Etiology
- Many.
- Cortical dysplasia.
- Hamartia.
- Stroke.
- Infection.
- Head trauma.
Syndromic:
Tumour:
- Dysembryoplastic neuroepithelial tumour.[2]
- Ganglioglioma.[3]
- Isomorphic astrocytoma.
Types
Features:[4]
- Temporal lobe epilepsy
- Mesial temporal sclerosis = scarring of the medial temporal lobe.
- Involves: hippocampus, parahippocampal gyrus and amygdala.
- Granule cell dispersion
Hamartia
- Small collection of ectopic glioneuronal cells.
- Morpholology resembling oligodendroglial-like cells. [5]
- Mostly amygdala, less common in hippocampus or temporal lobe.
- Can coexist with focal cortical dysplasia.
Focal cortical dysplasia (FCD)
- Localized malformations of the cortex.
- Frequently associated with epilepsy in children.
- Includes cortical dyslamination, cytoarchitectural changes and white matter abnormalities.
- Current consensus: ILAE classification scheme 2011 [6](based on previous classification by Palmini 2004):
- Type I FCD (focal)
- Ia: Abnormal radial cortical lamination.
- Ib: Abnormal tangential cortical lamination.
- Ic: Abnormal radial and tangential cortical lamination.
- Type II FCD (focal)
- IIa: Presence of dysmorphic neurons.
- IIb: Presence of dysmorphic neurons and balloon cells.
- Type III FCD (associated with other lesion)
- IIIa: FCD associated with hippocampal sclerosis.
- IIIb: FCD adjacent to a brain tumor.
- IIIc: FCD adjacent to vascular malformation.
- IIIc: FCD associated with previous injury (trauma, inflammation...).
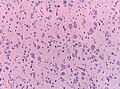
Dysmorphic neurons in FCD (HE)

Heterotopic neurons (NeuN)


Hippocampal sclerosis
- Most frequent histopathology in temporal lobe epilepsy (33% of all epilepsy surgery specimen).
- ILAE classification for hippocampus specimen:[7]
- ILAE type 1: cell loss predominantly in CA1 and CA4 sectors.
- ILAE type 2: predominant CA1 neuron loss and gliosis.
- ILAE type 3: CA4 predominant neuronal cell loss and gliosis.
Clinic: ILAE type 1: benefit from epilepsy surgery.
Notes:
- Gliosis withot neuronal loss is not considered hippocampal sclerosis.
Granule cell dispersion
- Affects dentate gyrus.
- Observed in up to 40% specimen with hippocampal sclerosis.
- Clinico-pathological classification:[8]
- Granule cell pathology (GCP) Type 1: Substantial granule cell loss.
- Granule cell pathology (GCP) Type 2: Cell dispersion, ectopic neurons or clusters of neurons in the molecular layer or bi-lamination.
Clinic:
- Association with longer epilepsy duration.
DDx:
- Epilepsy.
- Dementia.
Mild Malformation of Cortical Development with Oligodendroglial Hyperplasia
- Abbreviated: MOGHE [9].
- Frontal lobe.
- Nonlesional (3.7% of epilepsy case).
- Increase cellularity of Olig2-, and PDGFR-alpha-immunoreactive oligodendroglia.
Sudden unexpected death in epilepsy
- Abbreviated SUDEP.
Diagnosis:
- Negative autopsy.
- History of epilepsy.
Epidemiology:[10]
- Typically poorly controlled epilepsy.
- Incidence: 0.09-9 per 1000 patient-years.
See also
References
- ↑ URL: http://emedicine.medscape.com/article/342150-overview. Accessed on: 20 November 2010.
- ↑ Cataltepe, O.; Turanli, G.; Yalnizoglu, D.; Topçu, M.; Akalan, N. (Apr 2005). "Surgical management of temporal lobe tumor-related epilepsy in children.". J Neurosurg 102 (3 Suppl): 280-7. doi:10.3171/ped.2005.102.3.0280. PMID 15881751.
- ↑ Im, SH.; Chung, CK.; Cho, BK.; Lee, SK. (Mar 2002). "Supratentorial ganglioglioma and epilepsy: postoperative seizure outcome.". J Neurooncol 57 (1): 59-66. PMID 12125968.
- ↑ MUN. 15 November 2010.
- ↑ Kasper, BS.; Stefan, H.; Buchfelder, M.; Paulus, W. (Jan 1999). "Temporal lobe microdysgenesis in epilepsy versus control brains.". J Neuropathol Exp Neurol 58 (1): 22-8. PMID 10068310.
- ↑ Blümcke, I.; Aronica, E.; Miyata, H.; Sarnat, HB.; Thom, M.; Roessler, K.; Rydenhag, B.; Jehi, L. et al. (Mar 2016). "International recommendation for a comprehensive neuropathologic workup of epilepsy surgery brain tissue: A consensus Task Force report from the ILAE Commission on Diagnostic Methods.". Epilepsia 57 (3): 348-58. doi:10.1111/epi.13319. PMID 26839983.
- ↑ Blümcke, I.; Thom, M.; Aronica, E.; Armstrong, DD.; Bartolomei, F.; Bernasconi, A.; Bernasconi, N.; Bien, CG. et al. (Jul 2013). "International consensus classification of hippocampal sclerosis in temporal lobe epilepsy: a Task Force report from the ILAE Commission on Diagnostic Methods.". Epilepsia 54 (7): 1315-29. doi:10.1111/epi.12220. PMID 23692496.
- ↑ Blümcke, I.; Kistner, I.; Clusmann, H.; Schramm, J.; Becker, AJ.; Elger, CE.; Bien, CG.; Merschhemke, M. et al. (May 2009). "Towards a clinico-pathological classification of granule cell dispersion in human mesial temporal lobe epilepsies.". Acta Neuropathol 117 (5): 535-44. doi:10.1007/s00401-009-0512-5. PMID 19277686.
- ↑ Schurr, J.; Coras, R.; Rössler, K.; Pieper, T.; Kudernatsch, M.; Holthausen, H.; Winkler, P.; Woermann, F. et al. (01 2017). "Mild Malformation of Cortical Development with Oligodendroglial Hyperplasia in Frontal Lobe Epilepsy: A New Clinico-Pathological Entity.". Brain Pathol 27 (1): 26-35. doi:10.1111/bpa.12347. PMID 26748554.
- ↑ Tomson, T.; Nashef, L.; Ryvlin, P. (Nov 2008). "Sudden unexpected death in epilepsy: current knowledge and future directions.". Lancet Neurol 7 (11): 1021-31. doi:10.1016/S1474-4422(08)70202-3. PMID 18805738.