Difference between revisions of "Complex endometrial hyperplasia"
m |
|||
| (5 intermediate revisions by the same user not shown) | |||
| Line 13: | Line 13: | ||
| IF = | | IF = | ||
| Gross = thickened endometrium | | Gross = thickened endometrium | ||
| Grossing = | | Grossing = [[hysterectomy for endometrial hyperplasia grossing]] | ||
| Site = [[endometrium]] - see ''[[endometrial hyperplasia]] | | Site = [[endometrium]] - see ''[[endometrial hyperplasia]] | ||
| Assdx = [[obesity]] | | Assdx = [[obesity]], [[endometrium with squamous morules]] | ||
| Syndromes = | | Syndromes = | ||
| Clinicalhx = usu. premenopausal or perimenopausal | | Clinicalhx = usu. premenopausal or perimenopausal | ||
| Line 69: | Line 69: | ||
DDx: | DDx: | ||
*Artifactual gland crowding due to fragmentation - white space around the glands. | *Artifactual gland crowding due to fragmentation - white space around the glands. | ||
*Endometrial gland coiling - no sharp transition, moderate stroma between the glands horizontally. | *[[Endometrial gland coiling]] - no sharp transition, moderate stroma between the glands horizontally. | ||
*[[Endometrioid endometrial carcinoma]] - see ''[[endometrial carcinoma versus complex endometrial hyperplasia]]''. | *[[Endometrioid endometrial carcinoma]] - see ''[[endometrial carcinoma versus complex endometrial hyperplasia]]''. | ||
*Benign papillary proliferation of the endometrium.<ref name=pmid23211295>{{Cite journal | last1 = Ip | first1 = PP. | last2 = Irving | first2 = JA. | last3 = McCluggage | first3 = WG. | last4 = Clement | first4 = PB. | last5 = Young | first5 = RH. | title = Papillary proliferation of the endometrium: a clinicopathologic study of 59 cases of simple and complex papillae without cytologic atypia. | journal = Am J Surg Pathol | volume = 37 | issue = 2 | pages = 167-77 | month = Feb | year = 2013 | doi = 10.1097/PAS.0b013e318272d428 | PMID = 23211295 }}</ref> | |||
===Endometrial carcinoma versus complex endometrial hyperplasia=== | ===Endometrial carcinoma versus complex endometrial hyperplasia=== | ||
Complex endometrial hyperplasia: | Complex endometrial hyperplasia: | ||
| Line 115: | Line 115: | ||
Image: Endometrial polyp with fused glands -- high mag.jpg | Endometrial polyp with fused glands - high mag. (WC) | Image: Endometrial polyp with fused glands -- high mag.jpg | Endometrial polyp with fused glands - high mag. (WC) | ||
</gallery> | </gallery> | ||
www: | www: | ||
*[http://www.webpathology.com/image.asp?n= | *[http://www.webpathology.com/image.asp?n=3&Case=568 Complex endometrial hyperplasia without atypia (webpathology.com)]. | ||
*[http://www.webpathology.com/image.asp?n= | *[http://www.webpathology.com/image.asp?n=4&Case=568 Complex endometrial hyperplasia without atypia (webpathology.com)]. | ||
==Sign out== | ==Sign out== | ||
| Line 175: | Line 174: | ||
for the diagnosis of endometrial carcinoma. | for the diagnosis of endometrial carcinoma. | ||
</pre> | </pre> | ||
====Micro==== | |||
=====CEH with atypia===== | |||
The sections show endometrium with atypical hyperchromatic, densely packed branching glands. The nuclei of the atypical glands focally are round, 2-3x the size of a lymphocyte, and have grey/translucent chromatin and small nucleoli. No papillary or cribriform changes are appreciated. No desmoplastic stroma is identified. | |||
==See also== | ==See also== | ||
Latest revision as of 14:24, 2 March 2017
| Complex endometrial hyperplasia | |
|---|---|
| Diagnosis in short | |
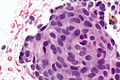
 Complex endometrial hyperplasia. H&E stain. | |
|
| |
| LM | increase in size & number of glands + irregular shape, nuclear pseudostratification, nuclear enlargement, mitoses common, +/-nuclear atypia (round nuclei ~ 2-3x the size of a lymphocyte, grey/translucent chromatin, nucleoli) |
| Subtypes | CEH NOS (CEH without atypia), CEH with atypia |
| LM DDx | endometrioid endometrial carcinoma, artifactual gland crowding |
| Gross | thickened endometrium |
| Grossing notes | hysterectomy for endometrial hyperplasia grossing |
| Site | endometrium - see endometrial hyperplasia |
|
| |
| Associated Dx | obesity, endometrium with squamous morules |
| Clinical history | usu. premenopausal or perimenopausal |
| Symptoms | abnormal uterine bleeding (AUB) |
| Prevalence | common |
| Clin. DDx | dysfunctional uterine bleeding (diagnosis of exclusion), endometrial carcinoma, atrophy, endometrial polyp, others |
| Complex endometrial hyperplasia | |
|---|---|
| External resources | |
| EHVSC | 10169 10181 (CEH with atypia) |
Complex endometrial hyperplasia, abbreviated CEH, is a relatively common pre-malignant pathology of the endometrium.
It is generally subdivided into complex endometrial hyperplasia without atypia and complex endometrial hyperplasia with atypia.
CEH with atypia is also known as complex atypical hyperplasia.
General
- Usually premenopausal or perimenopausal women.
- Associated with obesity.
- High risk of transformation to endometrial carcinoma especially when with atypia.
Gross
- Endometrial thickening.
Microscopic
Features:
- Increase in size & number of glands + irregular shape - key feature.
- Cell stratification.
- Nuclear enlargement.
- Mitoses common.
- +/-Nuclear atypia:
- Round nuclei ~ 2-3x the size of a lymphocyte.
- Grey/translucent chromatin.
- Nucleoli.
Notes:
- Normal "gland-to-stroma ratio" is 1:3.
- Two "touching" glands may be one gland in section.
- Atypical nuclei often hide between non-typical nuclei, like peg cells in the fallopian tube.
- Squamous morules commonly seen.
DDx:
- Artifactual gland crowding due to fragmentation - white space around the glands.
- Endometrial gland coiling - no sharp transition, moderate stroma between the glands horizontally.
- Endometrioid endometrial carcinoma - see endometrial carcinoma versus complex endometrial hyperplasia.
- Benign papillary proliferation of the endometrium.[1]
Endometrial carcinoma versus complex endometrial hyperplasia
Complex endometrial hyperplasia:
- Non-confluent - glands distinct from one another.
Classic criteria for endometrial carcinoma
This is pimping material that shows up on exams.
Endometrial carcinoma has one of the following:[2][3][4]
- Desmoplastic stromal response.
- Confluent cribriform growth. †
- Extensive papillary growth. †
- Severe cytologic atypia. †
Note:
- † There is a size cut-off for criteria 2, 3 and 4: > 2.1 mm.[3]
How to remember ABCDE:
- Atypia Bad.
- Confluent cribriform growth.
- Desmoplasia.
- Extensive papillary growth.
Images
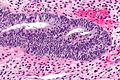
Complex endometrial hyperplasia:

CEH - low mag.

CEH - intermed. mag.

CEH - high mag.


Squamous morules - commonly associated with hyperplasia and malignancy:

SM - high mag.
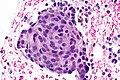
SM - very high mag.
SM - extremely high mag.



Fused glands suggestive of CEH in a polyp:
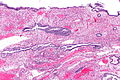
Endometrial polyp with fused glands - low mag. (WC)

Endometrial polyp with fused glands - intermed. mag. (WC)
Endometrial polyp with fused glands - high mag. (WC)



www:
- Complex endometrial hyperplasia without atypia (webpathology.com).
- Complex endometrial hyperplasia without atypia (webpathology.com).
Sign out
CEH without atypia
ENDOMETRIUM, BIOPSY: - COMPLEX ENDOMETRIAL HYPERPLASIA. -- NEGATIVE FOR CYTOLOGIC ATYPIA.
ENDOMETRIUM, BIOPSY: - SMALL FOCUS OF COMPLEX ENDOMETRIAL HYPERPLASIA WITHOUT ATYPIA, WITH SQUAMOUS MORULES. - ENDOMETRIAL POLYP WITH ONE ATYPICAL GLAND AND A SQUAMOUS MORULE. - SCANT ENDOCERVICAL EPITHELIUM WITHOUT APPARENT PATHOLOGY.
Hysterectomy
UTERUS AND CERVIX, TOTAL HYSTERECTOMY: - FOCAL COMPLEX ENDOMETRIAL HYPERPLASIA WITHOUT ATYPIA. - LEIOMYOMAS. - FIBROUS ADHESIONS. - UTERINE CERVIX WITHIN NORMAL LIMITS. - NEGATIVE FOR MALIGNANCY.
Micro
The sections show endometrium with pseudostratified glands and glandular dilation. On one section the gland-to-stroma ratio is increased and the glands are very focally back-to-back. Significant gland cribriforming is not identified. No nuclear atypia is apparent. Stromal desmoplasia is not identified.
CEH with atypia
Insufficient confluence for carcinoma
ENDOMETRIUM, BIOPSY: - COMPLEX ENDOMETRIAL HYPERPLASIA WITH ATYPIA, SEE COMMENT. COMMENT: The sections show architecturally complex crowded glands with focal morular squamous metaplasia and focal cribriforming. Desmoplasia is not identified. The degree of gland confluence is not considered sufficient for the diagnosis of endometrial carcinoma. Nuclear atypia is present focally.
Insufficient extent for carcinoma
ENDOMETRIUM, BIOPSY: - COMPLEX ENDOMETRIAL HYPERPLASIA WITH ATYPIA, SEE COMMENT. COMMENT: The sections show architecturally complex back-to-back glands with focal morular squamous metaplasia and cribriforming. Desmoplasia is not present. The extent, i.e. the size of the abnormality, is not considered sufficient for the diagnosis of endometrial carcinoma.
Micro
CEH with atypia
The sections show endometrium with atypical hyperchromatic, densely packed branching glands. The nuclei of the atypical glands focally are round, 2-3x the size of a lymphocyte, and have grey/translucent chromatin and small nucleoli. No papillary or cribriform changes are appreciated. No desmoplastic stroma is identified.
See also
References
- ↑ Ip, PP.; Irving, JA.; McCluggage, WG.; Clement, PB.; Young, RH. (Feb 2013). "Papillary proliferation of the endometrium: a clinicopathologic study of 59 cases of simple and complex papillae without cytologic atypia.". Am J Surg Pathol 37 (2): 167-77. doi:10.1097/PAS.0b013e318272d428. PMID 23211295.
- ↑ Nucci, Marisa R.; Oliva, Esther (2009). Gynecologic Pathology: A Volume in Foundations in Diagnostic Pathology Series (1st ed.). Churchill Livingstone. pp. 239. ISBN 978-0443069208.
- ↑ 3.0 3.1 Kurman, RJ.; Norris, HJ. (Jun 1982). "Evaluation of criteria for distinguishing atypical endometrial hyperplasia from well-differentiated carcinoma.". Cancer 49 (12): 2547-59. PMID 7074572.
- ↑ URL: http://www.cap.org/apps/docs/committees/cancer/cancer_protocols/2011/Endometrium_11protocol.pdf. Accessed on: 12 January 2012.