Difference between revisions of "Chondro-osseous tumours"
Jump to navigation
Jump to search
| Line 229: | Line 229: | ||
===Hypercalcemia DDx=== | ===Hypercalcemia DDx=== | ||
Mnemonic ''GRIMED'':<ref>TN06 Emerg</ref> | Mnemonic ''GRIMED'':<ref>TN06 Emerg</ref> | ||
*Granulomatous disease (tuberculosis, sarcoidosis). | *Granulomatous disease (tuberculosis, [[sarcoidosis]]). | ||
*Renal disease. | *Renal disease. | ||
*Immobility. | *Immobility. | ||
Revision as of 17:31, 29 September 2010
Bone occasionally crosses the desk of the pathologist. Primary bone tumours are rare; the most common bone tumour is metastases.[1]
Bone tumours occasionally are lumped with soft tissue tumours. Soft tissue tumours are dealt with in the soft tissue lesions article.
Normal
- Normal bone has osteocytes.
- If the osteocytes are missing... the bone is dead.
- Osteoblasts - make bone.
- Osteoclasts - destroy bone.
Memory device: 'b' before 'c'.
Diagnosing bone tumours
- Diagnosis should not be made without radiologic & clinical information.
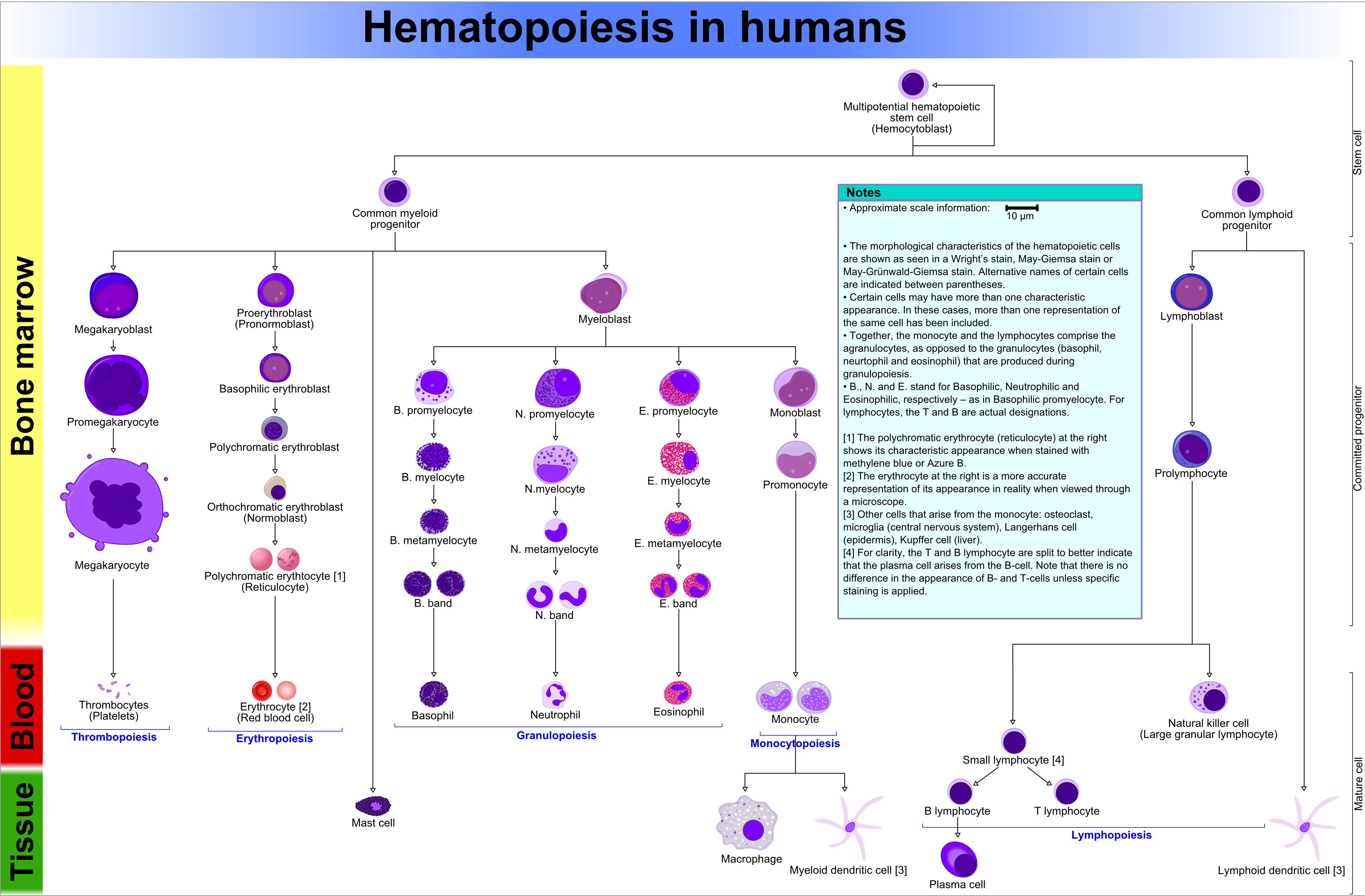
Bone marrow
- Fat content (%) ~= age (in years)[2]
- e.g. 60 year old will have 60% fatty replacement.
- Should see three cell lines.
- The cell lines:[3]
- Erythroid (red cells),
- Myeloid (white blood cells),
- Megakaryocytic (platelets).
- The cell lines:[3]
Note: Lymphocytes are considered separately and typically spared in bone marrow failure.[4]
Identifying the lines:[5]
- Megakaryocytes:
- Big cells ~ 3x the size of a RBC.
- Normoblasts (RBC precursors):
- Hyperchromatic, i.e. blue, nucleus.
- Myeloid line:
- Granules.
- Reniform nucleus, i.e. kidney bean shaped nucleus.
Images:
{kind=link}
Organization
- Mature hematopoeitic cells at the centre (distant from bone).
- Immature hematopoeitic cells adjacent to the bone.
Infectious
Osteomyelitis
General
- Hematogenous - often in children.
- Direct entry (skin defect) - adults with diabetes.
Microscopic
- PMNs.
Chronic osteomyelitis
- Plasma cells.
- May be sterile, i.e. no organisms.
Bone tumours
General
- Metastasis:primary bone tumours = >20:1.[1]
Common malignant
- Osteosarcoma.
- Chondrosarcoma.
- Ewing's sarcoma.
- Multiple myeloma.
- Metastases.
- Most common tumours metastatic to bone (mnemonic: BLT with Ketchup & Pickles):
- Breast.
- Liver.
- Thyroid.
- Kidney.
- Prostate.
- Most common tumours metastatic to bone (mnemonic: BLT with Ketchup & Pickles):
Epidemiology:[6]
- Osteosarcoma -> 2nd decade.
- Ewing's ->5-20 yrs.
- Chondrosarcoma -> from enchondroma or osteochrondroma -- patients over 40 yrs.
- Multiple myeloma -> most common primary bone tumour in adults.
Malignant bone tumours by age
Most common by age:[7]
- <1 year old - neuroblastoma.
- 1-10 years old - Ewing's of tubular bones.
- 10-30 years old - osteosarcoma, Ewing's of flat bones.
- 30-40 years old - reticulum cell sarcoma, fibrosarcoma, parosteal osteosarcoma, malignant giant cell tumour, lymphoma.
- >40 years old - mets, multiple myeloma, chondrosarcoma.
Benign aggressive bone tumours
- Giant cell tumours.
- Osteoblastoma.
- Thought to be related to osteoid osteoma.
- If in long bones often diaphyseal.
Giant cell tumour
General
Features:[10]
- Approximately 5% of primary bone tumours.
- Typical age: 20-45 years.
Clinical
- May present with joint pain, immobility.
Microscopic
Features:[11]
- Giant cells.
- Mononuclear cells, with nuclei similar to those in giant cells - key feature
Chondrosarcoma
Micro
Features:[12]
- Abnormal cartilage.
- Nuclear atypia.
- Nuclear clearing.
- Nucleoli.
Ewing sarcoma
General
- AKA EWS/PNET:
- EWS = Ewing sarcoma.
- PNET = Primative neuroectodermal tumour.
- EWS and PNET were once thought to be different tumours.
Clinical
- Painful.
- Usually younger than 20 years.
Radiology
Features:[13]
- Long bones, diaphyses.
- Destructive.
- "Onion-skin" periosteal reaction.
Microscopic
Classification:
- Small blue cell tumour.
Features:[14]
- Scant clear cytoplasm (contain glycogen - PAS +ve, PAS-D -ve).
- Lack nucleoli.
- Round small nucleus.
IHC
Features:[15]
- CD99 +ve (plasma membrane staining).
- CD45 -ve.
- Done to r/o lymphoma.
- +/-Neural markers (NSE, synaptophysin, CD57 (??? CD56 ???), S100).
- +/-Cytokeratins.
- Caveolin-1[16]
- New kid on the block.
Notes:[17]
- CD99 +ve (plasma membrane) tumours:
- Lymphoblastic lymphoma/leukemia.
- Angiomatoid fibrous histiocytoma.
- Desmoplastic small round cell tumour.
Molecular diagnostics
Common features:
- EWS/FLI-1 fusion gene formation due to translocation: t(11;22)(q24;q12).[18][19]
- Often detected by RT-PCR (with EWS 5' and FLI-1 3' primers).
Notes:
- The t(11;22)(q24;q12) is seen in ~90% of EWS/PNET... but also in:
- Olfactory neuroblastoma.
- Small cell osteogenic sarcoma.
- Polyphenotypic tumours.
- Rhbdomyosarcoma.
- Neuroblastoma (possibly).
- Several other translocations exist.
Osteosarcoma
General
- Terry Fox was afflicited by this tumour.
Definition
- Tumour that makes osteoid.
- Osteoid = (extracellular) organic component of bone, normally produced by osteoblasts (cells which make bone matrix).
Histology
- Spindle cells with malignant features (e.g. nuclear membrane irregularies, marked nuclear size differences, mitoses) surrounded by delicate strands of osteoid.
- Osteoid on H&E: pink, homogenous, "glassy".
- Tumours typically very cellular - when compared to normal bone.
- Large (multinucleated) osteoclast-like giant cells may be seen.[20]
Other
Pigmented villonodular synovitis
- Commonly abbreviated: PVNS.
- Course: benign.
Microscopic
Features:[21]
- Subsynovial nodules composed of cells with:
- Abundant cytoplasm.
- Pale nuclei.
- Multinucleated giant cells.
- Hemosiderin-laden macrophages.
- Foam cells.
Images:
{kind=link}
{kind=link}
Adamantinoma
General
Features:[13]
- Rare: < 1% of bone tumours.
- 25-35 years old.
- Tibia, fibula.
- Benign, may be locally aggressive.
- Cousin of ameloblastoma.[22]
Radiology
- Intracortical, radiolucent.
Microscopic
Features:
- Fibrous tumour.
Brown cell tumour
Etiology
- Due to hyperparathyroidism - usually parathyroid adenoma.
Microscopy
Features:
- Fibrosis.
Hypercalcemia DDx
Mnemonic GRIMED:[23]
- Granulomatous disease (tuberculosis, sarcoidosis).
- Renal disease.
- Immobility.
- Malignancy (esp. squamous cell carcinoma, plasmacytoma).
- Endocrine (primary hyperparathyroidism - leads to brown cell tumour).
- Drugs (thiazides ... others).
Osteoid osteoma
General
- Benign bone lesion.
Image:
See also
References
- ↑ 1.0 1.1 Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 632. ISBN 978-0781765275.
- ↑ IAV. 26 Feb 2009.
- ↑ http://emedicine.medscape.com/article/199003-overview
- ↑ http://emedicine.medscape.com/article/199003-overview
- ↑ http://upload.wikimedia.org/wikipedia/commons/6/69/Hematopoiesis_%28human%29_diagram.png
- ↑ TN05 OR42.
- ↑ TN05 OR42.
- ↑ TN05 OR41.
- ↑ URL: http://www.emedicine.com/RADIO/topic494.htm.
- ↑ Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 648. ISBN 978-0781765275.
- ↑ Klatt, Edward C. (2006). Robbins and Cotran Atlas of Pathology (1st ed.). Saunders. pp. 420. ISBN 978-1416002741.
- ↑ IAV. 26 February 2009.
- ↑ 13.0 13.1 Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 650. ISBN 978-0781765275.
- ↑ PST. 22 February 2010.
- ↑ Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 651. ISBN 978-0781765275.
- ↑ PST. 22 February 2010.
- ↑ PST. 22 February 2010.
- ↑ URL: http://atlasgeneticsoncology.org/Tumors/Ewing5010.html. Accessed on: 23 February 2010.
- ↑ PMID: 3163261
- ↑ Papalas JA, Balmer NN, Wallace C, Sangueeza OP (June 2009). "Ossifying dermatofibroma with osteoclast-like giant cells: report of a case and literature review". Am J Dermatopathol 31 (4): 379-83. doi:10.1097/DAD.0b013e3181966747. PMID 19461244.
- ↑ URL: http://www.wheelessonline.com/ortho/pigmented_villonodular_synovitis.
- ↑ NEED REF.
- ↑ TN06 Emerg
{kind=link}