Neuropathology
Neuropathology is the bane of many anatomical pathologists in teaching hospitals... 'cause they have to fill in for the neuropathologist when he or she is on vacation.
This article is an introduction to neuropathology. There are separate articles for brain tumours, the pituitary gland and muscle pathologies.
Gross
- Uncus (as in uncal herniation).
- Cerebellar tonsils (as in tonsillar herniation).
- Longitudinal fissure - divides cerebrum into hemispheres.
- Central sulcus - separate parietal lobe from frontal lobe.
- Lateral sulcus (Sylvian fissure).
Less important
- Glomeruli of Arnold.
- Over lies hippocampus.
Normal histology
Normal cells
- Neuron:
- Abundant cytoplasm - key feature.
- Often very large cells, with angled edges.
- Prominent nucleolus.
- Nissl substance (granular perinuclear material - rough ER).
- Glial cells.
- Oligodendrocyte.
- Small round nuclei (lymphocyte-like nucleus) - key feature.
- May resemble a fried egg on H&E (clear cytoplasm, central nucleus).
- Astrocyte.
- Irregular non-ovoid nucleus - key feature.
- Nuclei less dense than in oligodendrocyte.
- Close to blood vessels.
- Form blood-brain barrier.
- Cytoplasm normally not visible.
- Image: astrocyte (med.unsw.edu.au) (in endocrine development).
- Microglia - macrophage of the brain (derived from monocyte).
- May be large.
- May have vesicles.
- Oligodendrocyte.
- Ependyma.
- Simple ciliated cuboidal epithelium.
- Image: Ependyma (stonybrookmedicalcenter.org).
{kind=link}
{kind=link}
Normal cellular constituents in a table
| Key feature | Other features | Image | |
| Neuron | cytoplasm | Nissl substance (prominent RER), "sharp" corners in cell membrane |
red neurons (WC) |
| Astrocyte | non-ovoid nucleus | no cytoplasm | (unsw.edu) |
| Oligodendrocyte | round small nucleus | peri-nuclear clearing | |
| Microglia | rod-like shape, may have "bent" nucleus |
rarely seen in normal tissue | (ucsf.edu),(vcu.edu) |
{kind=link}
Neurons
There are many types of 'em. Broadly, they can be classified as:
- Pyramidal - have a pyramidal shape.
- Dentrites go to molecular layer.
- Axons go to outside of cortex.
- Non-pyramidal.
Motor neurons:
- Coarse Nissl substance - key feature.
- Nissl described as having a tigroid appearance.[1]
- Polygonal shape.
- Send dendrites in all directions.
Image: Motor neuron (stonybrookmedicalcenter.org).
{kind=link}
Histology - where
Subependyma
Features:[2]
- Ependyma (simple ciliated cuboidal epithelium).
- Subependymal plate - connective tissue with blood vessels.
Pons
Features:
- Looks like bacon.[3]
- Image: Pons (stonybrookmedicalcenter.org).
{kind=link}
Caudate
Features:
- Neurons with adjacent ependymal lining.[4]
- The caudate forms lateral wall of lateral ventricle.
Putamen
Features:
- Histologically identical to the caudate - but not adjacent to a ventricle, i.e. an ependymal lining.
- Striatopallidal fibers AKA pencils of Wilson - bundles of blue fibres (on H&E LFB).
Globus pallidus
Features:
- Histologically distinct from caudate and putamen.
Hippocampus
Hippocampal formation:[5]
- Dentate gyrus.
- "Dense" thin layer of nuclei.
- Quasi "U-shaped"; "open" (top) portion of "U" is superolateral.
- Image: Dentate gyrus (stonybrookmedicalcenter.org).
- Hippocampus proper (AKA Ammon's horn) - this is subdivided:
- CA3 - superior.
- CA1 - inferior (next to subiculum).
- CA2 - in between CA3 and CA1, lateral.
- CA4 - medial (closest to dentate gyrus; CA4 sits in "open" part of "U").
- Subicular complex.
{kind=link}
Images:
- Hippocampus - frontal section (WP).
- Hippocampus - good schematic (WC).
- Hippocampus (ajnr.org).
- Hippocampus and subiculum (hu-berlin.de).
- Hippocampus - crappy schematic (ucsd.edu).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Important note:
- CA1 - weak link, dies in ischemia, affected by hypoglycemia.
- CA2 - resistant to ischemia.
DDx of ischemia-like changes in the hippocampus:
- Toxins.
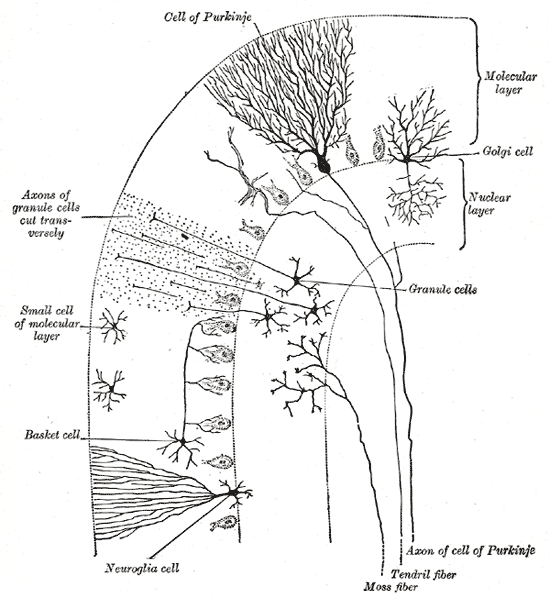
Cerebellum
Main components:
- Cortex (superficial) - branches (Christmas tree-like).
- Dentate nucleus (deep) - looks like the bite impression of a molar.
{kind=link}
Cerebellar cortex:
- Layers (superficial to deep) - mnemonic MPG:[6]
- Molecular layer -- "very pink" on H&E.
- Inhibitory interneurons: stellate cells, basket cells.
- Purkinje cell layer.
- One cell layer thick - hueuege cells.
- Granule cell layer -- "very blue" on H&E.
- Granule cells (many), interneurons (Golgi cells --few in number). (???)
- Molecular layer -- "very pink" on H&E.
- Images:
{kind=link}
{kind=link}
Cerebral cortex
Layers (superficial to deep):
- Molecular layer.
- Empty appearing.
- Outer granular layer.
- Outer pyramidal layer.
- Inner granular layer.
- Not prominent in frontal cortex.
- Where the thalamic axons end.
- Inner pyramidal layer.
- Location of Betz neurons - large motor neurons of cerebral cortex.
- Polymorphic layer.
Images:
{kind=link}
{kind=link}
{kind=link}
Histopathology
- Reactive astrocytes.
- Eosinophilic cytoplasm.
- Peripheral nucleus.
- Well-defined cell border.
- Many branching processes.
Alzheimer type II astrocytes:[7]
- Large cleared nuclei.
- Indistinct cytoplasm.
- Images:
{kind=link}
{kind=link}
- Axonal swellings
- Image: Axonal swelling - neuropathologyweb.org.
{kind=link}
Architecture
- Rosette = circular/flower-like arrangement of cells[8]
- Pseudorosette = circular/flower-like arrangement of cells with blood vessel at the centre[8]
- Rosenthal fibres = worm-like or corkscrew-like eosinophilic bodies.
- Image: Rosenthal fibres - wikipedia.org.
- Pseudopallisading
{kind=link}
Notes: Good set of articles - [9]
Ring enhancing lesions
In HIV/AIDS patients... mass on CT if infection:
- Toxoplasmosis - most common.[10]
Ring enhancing lesion (DDx) - mnemonic MAGICAL DR:[11]
- Metstasis.
- Abscess.
- Glioblastoma.
- Infarct.
- Contusion.
- AIDS-related.
- Lymphoma + HIV assoc. disease (toxoplasma).
- Demyelination (e.g. multiple sclerosis).
- Resolving hematoma.
Alcohol & CNS
Pathology:[12]
- Morel's laminar sclerosis
- central pontine myelinolysis
- Wernicke's encephalopathy
- Mnemonic WACO:
- Wernicke's.
- Ataxia.
- Confusion, confabulation -- Korsakoff.
- Ocular Sx (CN IV palsy).
- Cause: thiamine deficiency.
- Mnemonic WACO:
- Mammillary body shrinkage.[13]
Non-tumour
Acute disseminated encephalomyelitis
General
- Thought to be autoimmune.
- May mimic multiple sclerosis.
- Abbreviated "ADEM".
Diagnosis
- Need to r/o infection (with lumbar puncture).
- No old plaques on imaging (MRI).
Microscopic
Features:
- Spares subcortical fibres (???)
Tx
- Steroids.
- Plasmapheresis.
DDx
- Multiple sclerosis.
Cysts
General
- All are "benign", but some may be fatal due to spatial constraints.
List of cysts
- Colloid cyst.[14]
- Columnar epithelium.
- Arachnoid cyst - considered precursor of meningioma.
- Psammoma bodies.
- Clumps of cells.
- Whorled pattern.
- Dermoid cyst.
- Skin + adnexal structures.
- ... think of ovarian dermoid.
- Epidermoid.
- Choriod cyst.
- ?
- Neuroenteric cyst.
- Epithelial cyst.
Dementia
- Alzheimer's dementia.
- Vascular.
- multi-infarct dementia.
- Parkinson's associated dementia.
- Lewy body dementia.
- Alcohol-related dementia.
- Fronto-temporal dementia (Pick disease).
- Multisystem atrophy.
Mnemonic VITAMIN D VEST:[15]
- Vitamin deficiency (B12, folate, thiamine).
- Infection (HIV).
- Trauma.
- Anoxia.
- Metabolic (Diabetes).
- Intracranial tumour.
- Normal pressure hydrocephalus.
- Degenerative (Alzheimer's, Huntington's, CJD).
- Vascular.
- Endocrine.
- Space occupying lesion (chronic subdural hematoma).
- Toxins (alcohol).
Lewy body dementia
- Parkinsonian features.
- Hallucinations (visual).
- Progressive cog. decline with fluctuations.
Multiple system atrophy
Brain tumours
Tumours are a big part of neuropathology.
Paediatric pathology
Joubert syndrome
- Malformation of the cerebellar vermis.[18]
Epidemiology
- Autosomal recessive - mutation in a number of genes including NPHP1, AHI1, and CEP290.[18]
Histiocytoses
Features of histiocytoses:[19]
| Histologic features | EM features | CD68 | S-100 | CD1a | |
|---|---|---|---|---|---|
| Macrophage | epithelioid cells, giant cells | - | + | - | - |
| Erdheim-Chester disease | Touton giant cells | - | + | +/- | - |
| Rosai-Dorfman | Emperipolesis | - | + | + | - |
| Langerhans-histiocytosis | Reniform nuclei, eosinophilic cytoplasm |
Birbeck granules | + | + | + |
Stroke
Gross
- Soft/mushy brain.
- Older infarcts.
- A "roof" is present - a thin submeningeal layer is preserved by the CSF.[20]
- "Roof" is absent in trauma.
- Cavity - in older infarcts.
- Multiple sclerosis does not cavitate.
- A "roof" is present - a thin submeningeal layer is preserved by the CSF.[20]
Global ischemia
General
- Often due to cardiac arrest.
Microscopic
Features:
- Hippocampal ischemic changes:
- Loss of neurons in CA1, CA3 and CA4 +/- "cavitation".
- Neuronal loss: No blue (nuclei) where there should be some.
- Cavitation: bubbles/clear spaces where there should be none.
- CA2 neurons preserved.
- Loss of neurons in CA1, CA3 and CA4 +/- "cavitation".
Multiple sclerosis
General
- A bread 'n butter disease of neurology in Canada.
Radiologic/Gross
Features:[21]
- White matter lesions.
- Cerebrum (classically): periventricular distribution.
- Optic nerves (optic neuritis) - classic presentation.
Microscopic
Features:[22]
- Perivascular inflammation.
- Demyelination.
- Subcortical myelinated fibers are often spared.
Classification of MS lesions:
- Early active.
- Inactive.
- Early remyelinating.
- Late remyelinating.
Weird stuff
Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL)
General
- Autosomal dominant disorder - the name implies.[23]
- Cases strokes in 40-50 year-old.
- Characteristic MRI findings - present in asymptomatic individuals with mutation.
Etiology
- Mutation of Notch 3 gene.[24]
Diagnosis
- Proven Notch 3 mutation.
- Can be diagnosed on a skin biopsy.
- IHC for Notch 3 -- +ve staining in Notch 3 mutants.
Histology
Features:
- Subcortical infarcts.
- Patches of (non-myelinated) tissue within the white matter deep to the cortex with abundant macrophages.
Note:
- No cortical involvement -- this is unlike multiple sclerosis.
DDx:
- Amyloidosis.
- Binswanger's disease - multi-infarct dementia affecting subcortical white matter.
- Often diagnosed as Alzheimer's disease in the past.
Electron microscopy
- Granular osmiophilic material (GOM).
Binswanger's disease
General
- Multi-infarct dementia affecting subcortical white matter.
- Waste-basket diagnosis; diagnosed if CADASIL and amyloidosis have been excluded.
- Diagnosis has been controversial -- most with this entity (in the past) were diagnosed with Alzheimer's disease.
Microscopic
Features:
- Subcortical lesions that replace the myelin consisting of macrophages.
See also
References
- ↑ URL: http://www.stonybrookmedicalcenter.org/pathology/neuropathology/chapter1. Accessed on: 5 July 2010.
- ↑ Half-day. 28 June 2010.
- ↑ Half-day. 28 June 2010.
- ↑ URL: http://www.stonybrookmedicalcenter.org/pathology/neuropathology/chapter1. Accessed on: 2 July 2010.
- ↑ URL: http://www.stonybrookmedicalcenter.org/pathology/neuropathology/chapter1. Accessed on: 2 July 2010.
- ↑ URL: http://www.stonybrookmedicalcenter.org/pathology/neuropathology/chapter1. Accessed on: 2 July 2010.
- ↑ URL: http://www.neuropathologyweb.org/chapter1/chapter1bAstrocytes.html. Accessed on: 2 July 2010.
- ↑ 8.0 8.1 PMID 16551982
- ↑ http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=PureSearch&db=PubMed&details_term=Neuropathology%20for%20the%20neuroradiologist
- ↑ MUN. Feb 3, 2009.
- ↑ TN2005 NS7.
- ↑ http://www.journals.elsevierhealth.com/periodicals/ycdip/article/S0968-6053(07)00035-X/abstract
- ↑ Shear PK, Sullivan EV, Lane B, Pfefferbaum A (November 1996). "Mammillary body and cerebellar shrinkage in chronic alcoholics with and without amnesia". Alcohol. Clin. Exp. Res. 20 (8): 1489-95. PMID 8947329. http://www3.interscience.wiley.com/resolve/openurl?genre=article&sid=nlm:pubmed&issn=0145-6008&date=1996&volume=20&issue=8&spage=1489.
- ↑ MUN. 11 Mar 2009.
- ↑ TN06 PS19
- ↑ Wenning, GK.; Stefanova, N.; Jellinger, KA.; Poewe, W.; Schlossmacher, MG. (Sep 2008). "Multiple system atrophy: a primary oligodendrogliopathy.". Ann Neurol 64 (3): 239-46. doi:10.1002/ana.21465. PMID 18825660.
- ↑ Uversky, VN. (Oct 2008). "Alpha-synuclein misfolding and neurodegenerative diseases.". Curr Protein Pept Sci 9 (5): 507-40. PMID 18855701.
- ↑ 18.0 18.1 http://www.ninds.nih.gov/disorders/joubert/joubert.htm
- ↑ Sternberg Surg. Path. P.479.
- ↑ MUN. 16 December 2009.
- ↑ URL: http://library.med.utah.edu/kw/ms/path.html. Accessed on: 12 July 2010.
- ↑ URL: http://library.med.utah.edu/kw/ms/path.html. Accessed on: 12 July 2010.
- ↑ Tikka, S.; Mykkänen, K.; Ruchoux, MM.; Bergholm, R.; Junna, M.; Pöyhönen, M.; Yki-Järvinen, H.; Joutel, A. et al. (Apr 2009). "Congruence between NOTCH3 mutations and GOM in 131 CADASIL patients.". Brain 132 (Pt 4): 933-9. doi:10.1093/brain/awn364. PMID 19174371.
- ↑ Kalaria, RN.; Viitanen, M.; Kalimo, H.; Dichgans, M.; Tabira, T. (Nov 2004). "The pathogenesis of CADASIL: an update.". J Neurol Sci 226 (1-2): 35-9. doi:10.1016/j.jns.2004.09.008. PMID 15537516.