Extramammary Paget disease
| Extramammary Paget disease | |
|---|---|
| Diagnosis in short | |
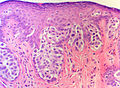
 Extramammary Paget's disease. H&E stain. | |
|
| |
| LM | large epithelioid cells - nested or single - in the epidermis, clear/pale cytoplasm (occasionally eosinophilic), large nucleoli |
| LM DDx | benign Toker cell hyperplasia, malignant melanoma, Bowen's disease, apocrine carcinoma of the skin |
| IHC | CK7 +ve, CEA +ve, S-100 -ve, CK5/6 -ve, HER2 +ve |
| Gross | erythema, +/-weeping, +/-crusted |
| Site | vulva, penis, scrotum, others |
|
| |
| Symptoms | pruritis (itchy) |
| Prognosis | typically benign - usually not associated with an underlying malignancy (unlike Paget's disease of the breast) |
| Clin. DDx | contact dermatitis, lichen sclerosus |
Extramammary Paget disease, abbreviated EMPD, is a skin disease. As the name suggests, there is also a Paget disease of the breast.
There is also a Paget disease of the bone - just to make things confusing. This is dealt with in the bone article and has nothing (from a pathologic perspective) to do with the Paget disease discussed in this article
General
- Two types
- Primary Extramammary Paget disease - a malignancy of the cutaneous apocrine glands
- Arises in apocrine rich areas - usually the vulva but also the groin, inguinal area, perineum, penis[1] or scrotum.[2] and rarely axilla or eye.
- Usually entirely intraepidermal but may be associated with an underlying apocrine gland carcinoma (in contrast to mammary Paget disease which is usually associated with underlying mammary carcinoma).
- Secondary Extramammary Paget disease - intraepidermal spread from a distant tumor
- Usually of urothelial or colorectal origin.
- Arises in the perineal areas near these organs
- Primary Extramammary Paget disease - a malignancy of the cutaneous apocrine glands
Clinical:
- Pruritis.
- R/O VIN
- R/O vulvitis
Gross
Features:[2]
- Plaque with an irregular border.
- Erythematous or white.
Clinical DDx:
- Lichen sclerosus.[3]
- Vulvar intraepithelial neoplasia
- Vulvar squamous cell carcinoma in situ
- Other vulvitis
Images
Microscopic
Features:
- Epitheliod morphology (round/ovoid).
- Cells nested or single.
- Classically Paget cells ride above the basal cell layer
- But the process can fill the entire epidermis
- Clear/pale cytoplasm key feature - may also be eosinophilic.
- Large nucleoli.
Images

Anus Pagets Disease - (SKB)
Anus Pagets Disease - (SKB)

Anus Pagets Disease - (SKB)



{kind=link}
{kind=link}
DDx
- Malignant melanoma in situ.
- Bowen disease - Pagetoid squamous cell carcinoma in situ.
- Pagetoid vulvar intraepithelial neoplasia
- Vulvar squamous cell carcinoma.
Notice that mammary Paget disease and Toker cell hyperplasia are not part of this DDX (wrong locations) except possibly in the rare case of EMPD arising in the axilla where mammary arising from a ectopic nipple or ectopic breast tissue may be a consideration. Notice that EMPD is not really part of the DDX of pagetoid cutaneous squamous cell carcinoma arising on typical sun damaged skin (arm, cheek, leg) - if it's from an apocrine rich area - it's not EMPD.
Stains
- Mucicarmine stain +ve.
IHC
- Extramammary Paget disease is a 'big' diagnosis in that the diagnosis will have significant clinical consequences. So a large panel of immuno is required to nail down the diangosis.
- Is the lesion epithelial or melanocytic? (S100, Melan A)
- Is the lesion adenocarcinoma or squamous cell carcinoma?
- Low molecular weight (CK7, cam5.2) or high molecular weight keratins (34BE12, CK5/6)?
- Adenocarcinoma markers? - CEA, BerEP4
- Nuclear differentiation markers? - p63 (squamous) vs GATA3 (adnexal)
- Is the lesion primary or secondary?
- Secondary extramammary Paget disease may be CK20 positive (urothelial or rectal)
- If CK20 is positive are other organ specific markers positive? - CDX2 - colorectal or GATA3 - urothelial
Panel:
- A carcinoma marker - CEA or BerEP4 or both
- Differential keratins - low molecular weight (glandular) cam5.2, CK7 vs high molecular weight (squamous) 34BE12, CK5/6[4]
- CK7 and CK20 - where does it come from?
- S100 and Melan A - exclude melanoma in situ
- Differentiation markers GATA - apocrine and urothelial; p63 - squamous, CDX2 - colorectal
- Notice that a CK20 negative urothelial origin EMPD will show the same immunoprofile as a primary cutaneous EMPD.
- Notice that you do not need to include markers for mammary Paget disease or Toker cells.
You can not rely on any one marker - a panel is required
See also
References
- ↑ Ekwueme, KC.; Zakhour, HD.; Parr, NJ. (2009). "Extramammary Paget's disease of the penis: a case report and review of the literature.". J Med Case Reports 3: 4. doi:10.1186/1752-1947-3-4. PMID 19126202.
- ↑ 2.0 2.1 2.2 Guerra, R.; Misra, S. (2013). "Management of Extramammary Paget's Disease: A Case Report and Review of the Literature.". Case Rep Dermatol Med 2013: 436390. doi:10.1155/2013/436390. PMID 24349803.
- ↑ Bansal, D.; Bowman, CA. (Feb 2004). "Extramammary Paget's disease masquerading as lichen sclerosus.". Int J STD AIDS 15 (2): 141-2. doi:10.1258/095646204322764361. PMID 15006079.
- ↑ RS. May 2010.
- ↑ Raju, RR.; Goldblum, JR.; Hart, WR. (Apr 2003). "Pagetoid squamous cell carcinoma in situ (pagetoid Bowen's disease) of the external genitalia.". Int J Gynecol Pathol 22 (2): 127-35. PMID 12649666.
- ↑ Sah, SP.; McCluggage, WG. (Mar 2013). "Florid vulval Paget disease exhibiting p16 immunoreactivity and mimicking classic VIN.". Int J Gynecol Pathol 32 (2): 221-7. doi:10.1097/PGP.0b013e31825909f6. PMID 23370646.