Renal oncocytoma
| Renal oncocytoma | |
|---|---|
| Diagnosis in short | |
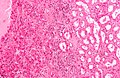
 Renal oncocytoma. H&E stain. | |
|
| |
| LM | abundant eosinophilic cytoplasm - slightly granular, cells arranged in nests, nuclei uniform and round without significant pleomorphism |
| LM DDx | chromophobe renal cell carcinoma eosinophilic variant, clear cell renal cell carcinoma eosinophilic variant, papillary renal cell carcinoma oncocytic variant |
| Stains | Hale's colloidal iron -ve |
| IHC | CK7 -ve/cytoplasmic +ve |
| EM | abundant mitochondria |
| Gross | mass, mahogany brown +/- central scar |
| Site | kidney - see kidney tumours |
|
| |
| Radiology | central scar |
| Prognosis | benign |
| Clin. DDx | other kidney tumours |
Renal oncocytoma is a benign kidney tumour that is removed to exclude malignancy.
General
- Can be difficult to distinguish radiologically from RCC (chromophobe subtype).
- ... and pathologists occasionally struggle like the radiologists.
- Benign tumour - the reason it is excised is... one cannot be certain it isn't a RCC.
Gross
- Mass, mahogany brown.
- Well circumscribed.
- 1/3 have a characteristic central scar.[1]
Image

Renal oncocytoma with central scar. (WP)

Microscopic
Features:
- Eosinophilic cytoplasm - slightly granular key feature.
- Cells arranged in nests.
- Nuclei uniform and round.[1]
- Slightly enlarged nuclei, but no significant pleomorphism (size variation) - important.
Notes:
- May look like eosinophilic variant of chromophobe RCC -- this is the main DDx.
- A comparison based on histomorphology: Tabular comparison between ChRCC & oncocytoma.
- Oncocytoma typically has: no perinuclear clearing, no raisinoid nuclei, no binucleation.
- A comparison based on histomorphology: Tabular comparison between ChRCC & oncocytoma.
DDx:
- Chromophobe renal cell carcinoma, eosinophilic variant.
- Clear cell renal cell carcinoma, eosinophilic variant.
Images
Oncocytoma - high mag. (WC/Nephron)
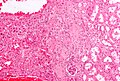
Oncocytoma - intermed. mag. (WC/Nephron)

Oncocytoma - low mag. (WC/Nephron)


Stains
- Hale's colloidal iron -ve.
- ChRCC +ve (blue granular cytoplasmic).
IHC
- CK7 -ve[2]/+ve (cytoplasmic) .
- Chromophobe renal cell carcinoma = cell membrane +ve.
- PAX2 +ve .[3]
- Oncocytoma 20 of 23 +ve versus ChRCC 1 of 11 +ve.
- Amylase α-1A +ve.[4]
Sign out
Biopsy
KIDNEY MASS, RIGHT, CORE BIOPSY: - RENAL TUMOUR WITH ONCOCYTIC CYTOPLASM, FAVOUR ONCOCYTOMA.
Micro
The sections show a tumour with cells arranged in nests. The tumour cells have abundant eosinophilic cytoplasm. The tumour cell nuclei are predominantly round. No perinuclear halos are apparent. Binucleation is not common. No zonal necrosis is identified. Focally, tumour nests are spaced reminiscent of an archipelago. Mitoses are not apparent. The tumour is moderately circumscribed.
A small amount of renal parenchyma is present. No definite glomeruli are identified. No significant interstitial fibrosis is present. No inflammation is apparent.
Resection
PORTION OF KIDNEY, RIGHT, PARTIAL NEPHRECTOMY: - ONCOCYTOMA.
Micro
The sections show a tumour with cells arranged in nests. The tumour cells have abundant eosinophilic cytoplasm. The tumour cell nuclei are round and have round nucleoli. No perinuclear halos are apparent. Binucleation is not apparent. No zonal necrosis is identified. Focally, tumour nests are spaced reminiscent of an archipelago. Mitoses are not apparent. The tumour is moderately circumscribed.
The thin rim of renal parenchyma has no apparent pathology on the H&E stained sections.
See also
References
- ↑ 1.0 1.1 Zhou, Ming; Magi-Galluzzi, Cristina (2006). Genitourinary Pathology: A Volume in Foundations in Diagnostic Pathology Series (1st ed.). Churchill Livingstone. pp. 302. ISBN 978-0443066771.
- ↑ Liu, L.; Qian, J.; Singh, H.; Meiers, I.; Zhou, X.; Bostwick, DG. (Aug 2007). "Immunohistochemical analysis of chromophobe renal cell carcinoma, renal oncocytoma, and clear cell carcinoma: an optimal and practical panel for differential diagnosis.". Arch Pathol Lab Med 131 (8): 1290-7. doi:10.1043/1543-2165(2007)131[1290:IAOCRC]2.0.CO;2. PMID 17683191.
- ↑ Memeo L, Jhang J, Assaad AM, et al. (February 2007). "Immunohistochemical analysis for cytokeratin 7, KIT, and PAX2: value in the differential diagnosis of chromophobe cell carcinoma". Am. J. Clin. Pathol. 127 (2): 225–9. doi:10.1309/9KWEA4W9Y94D1AEE. PMID 17210525. http://ajcp.ascpjournals.org/cgi/pmidlookup?view=long&pmid=17210525.
- ↑ Jain, S.; Roy, S.; Amin, M.; Acquafondata, M.; Yin, M.; Laframboise, W.; Bastacky, S.; Pantanowitz, L. et al. (Dec 2013). "Amylase α-1A (AMY1A): A Novel Immunohistochemical Marker to Differentiate Chromophobe Renal Cell Carcinoma From Benign Oncocytoma.". Am J Surg Pathol 37 (12): 1824-30. doi:10.1097/PAS.0000000000000108. PMID 24225843.