Keratoacanthoma
Keratoacanthoma is clinically worrisome lesion that classically arise on the nose. It is abbreviated KA.
General
- Generally considered to be benign.
- Rare reports of metastases suggesting it may be a form of squamous cell carcinoma.[1]
Clinical
- May grow rapidly (weeks or months) then involute.
- Main DDx is squamous cell carcinoma.
- Exophytic lesion, well-circumscribed.
Gross
- Raised dome-like lesions with a central crater-like defect.

Keratoacanthoma. (WC)

Microscopic
Features:[2]
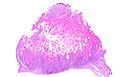
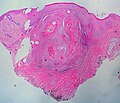
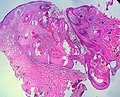
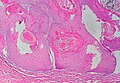
- Expansion of stratum spinosum - pushing tongue-like downward growth of epidermis into the dermis.
- Keratin collection ("keratin plug") at the center of lesion-superficial aspect.
- Cells have glassy pink cytoplasm.
- Minimal/no nuclear atypia.
Note:
- Classically described as a "volcano lesion" with pale pink cells.
- May have features of regression - PMNs, fibrosis (???).
DDx:[3]
- Verruca vulgaris.
- Conventional squamous cell carcinoma of the skin with a cup-shape.
- Pseudoepitheliomatous hyperplasia.
Image
Keratoacanthoma. (WC)
Keratoacanthoma. (WC/euthman)
Keratoacanthoma. (WC/euthman)
Keratoacanthoma. (WC/euthman)

,_H%26E.jpg)
,_H%26E.jpg)
,_H%26E.jpg)
Sign out
LESION, LEFT SIDE OF NOSE, EXCISION: - KERATOACANTHOMA. - SOLAR ELASTOSIS.
Micro
The sections show hair-bearing skin with a dome-shaped lesion that consists of a cup-shaped epidermal rim, and a large plug of keratin. The lesion is surrounded by a mild patchy lymphoplasmacytic infiltrate. No mitotic activity is apparent. The keratinocytes have minimal atypia and mature to the surface. A granular layer is present. The lesion is completely excised in the plane of section.
There is no hypergrlanulosis. No koilocytes are seen. Solar elastosis is present.
See also
References
- ↑ Mandrell JC, Santa Cruz D (August 2009). "Keratoacanthoma: hyperplasia, benign neoplasm, or a type of squamous cell carcinoma?". Semin Diagn Pathol 26 (3): 150–63. PMID 20043514.
- ↑ Klatt, Edward C. (2006). Robbins and Cotran Atlas of Pathology (1st ed.). Saunders. pp. 378. ISBN 978-1416002741.
- ↑ Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 379. ISBN 978-0443066542.