Difference between revisions of "Neuropathology"
m (→Microscopic: fix link to image) |
m (→Astrocyte changes: wikify, gr.) |
||
| Line 80: | Line 80: | ||
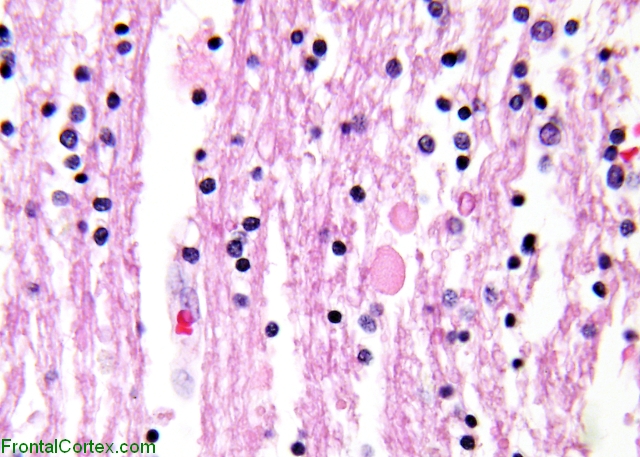
*Cellular processes loaded with tau protein (as may be seen with tau [[IHC]] or Gallyas silver stain); Parisian-star-like appearance with special stain. | *Cellular processes loaded with tau protein (as may be seen with tau [[IHC]] or Gallyas silver stain); Parisian-star-like appearance with special stain. | ||
*+/-Multinucleated. | *+/-Multinucleated. | ||
* | *A classic feature of ''[[progressive supranuclear palsy]]''. | ||
====Other glial==== | ====Other glial==== | ||
Revision as of 16:50, 2 March 2011
Neuropathology is the bane of many anatomical pathologists in teaching hospitals... 'cause they have to fill in for the neuropathologist when he or she is on vacation.
This article is an introduction to neuropathology. There are separate articles for brain tumours, the pituitary gland, the spine, muscle pathologies, neurohistology and neuroanatomy.
Neuroanatomy
This is a large topic. It covered in a separate article, that also covers grossing.
Neuroradiology
Enhancing vs. non-enhancing:
- If it is tumour... enhancing usu. high grade, non-enhancing usu. low grade.
Ring enhancing lesions
In HIV/AIDS patients... mass on CT if infection:
- Toxoplasmosis - most common.[1]
Ring enhancing lesion (DDx) - mnemonic MAGICAL DR:[2]
- Metstasis.
- Abscess.
- Glioblastoma.
- Infarct.
- Contusion.
- AIDS-related.
- Lymphoma + HIV assoc. disease (toxoplasma).
- Demyelination (e.g. multiple sclerosis).
- Resolving hematoma.
Grossing
This is covered in the neuroanatomy article.
Gross pathology
The gross usually useless for arriving at a definitive diagnosis.
Exceptions:[3]
- Sausage shape lesion of filum terminale = myxopapillary ependymoma.
- Soft & tan colour = pituitary adenoma.
Normal histology
This is a big topic. It is covered in a separate article called neurohistology.
Histopathology
Neuronal changes
- Central chromatolysis.[4]
Images:
- Central chromatolysis - intermed. mag. (WC).
- Central chromatolysis - NF stain - very high mag. (WC).
{kind=link}
{kind=link}
Glial changes
Astrocyte changes
Reactive astrocytes:
- Approximately equally-spaced; distance between neighbouring astrocytes is ~2x (or more) the cell size.
- Well-defined cell border.
- Eosinophilic cytoplasm with many branching processes.
- Classically described as "funnel-shaped" in benign astrocytes.[7]
- Peripheral nucleus.
- Image: Reactive astrocytes - high mag. (WC).
{kind=link}
Alzheimer type II astrocyte:[8]
- Large cleared nucleus - key feature.
- Indistinct cytoplasm.
- Found in the context of hepatic encephalopathy in basal ganglia and lower layers of cortex.[9]
- Images:
{kind=link}
{kind=link}
Creutzfeldt cell:[10]
- Astrocyte that mimics a mitoses; has moderate (identifiable) cytoplasm.
- Finding associated with demyelinating disease.
Gemistocytic astrocytes:[11]
- Distinct eosinophilic cytoplasm - with ground-glass appearance.
Tufted astrocytes:[12]
- Cellular processes loaded with tau protein (as may be seen with tau IHC or Gallyas silver stain); Parisian-star-like appearance with special stain.
- +/-Multinucleated.
- A classic feature of progressive supranuclear palsy.
Other glial
Bergmann gliosis (in the cerebellum):[10]
- Thin layer of cells (2-3 cells), nuclei open and larger than granular cell layer nuclei.
{kind=link}
{kind=link}
{kind=link}
Reactive change vs. malignancy
Reactive changes vs. malignancy (mnemonic MIMICS):[13]
- MIcrovesicular pattern.
- Mitoses.
- Irregular spacing.
- Calcifications.
- Satellitosis, perineuronal.
- Large "crowds" of glial cells associated with nuclei.
Architecture
All things rosette
- Rosette = circular/flower-like arrangement of cells.[14]
- Perivascular pseudorosette = circular/flower-like arrangement of cells with blood vessel at the centre.[14]
- Ependymoma.
- Medulloblastoma, PNET.
- Central neurocytoma.
- Glioblastomas
- Homer-Wright rosette = (circular) rosette with a small (~100 micrometers ???) meshwork of fibers (neuropil) at the centre.[14]
- Medulloblastoma.
- Image: Medulloblastoma (ouhsc.edu).[15]
- PNET (can be thought of as a supratentorial medulloblastoma) .
- Medulloblastoma.
{kind=link}
- Flexner-Wintersteiner rosette = rosette with empty centre (donut hole).[14]
- Retinoblastomas.
- Pineoblastomas.
- Medulloepitheliomas.
- True ependymal rosette = surrounds a space.[14]
- Ependymoma.
- Pineocytomatous/neurocytic rosette = irregular rosette with a large meshwork of fibers (neuropil) at the centre.[14]
- Similar to Homer-Wright rosette.
- Pineocytoma.
- Neurocytoma.
Other
- Rosenthal fibres = worm-like or corkscrew-like (brightly) eosinophilic bodies; 10-40 micrometers.
- Key feature: variable thickness; helps separate from RBCs.
- Well-seen on trichrome stains.
- Images: Rosenthal fibres (WP), Rosenthal fibres - smear (WC/AFIP).
- Eosinophilic granular bodies = related to Rosenthal fibres; round cytoplasmic hyaline droplets in astrocytes.[16]
- Image: EGBs (WC/AFIP).
- Pseudopalisading - picket fence-like alignment of cells; long axis of cells perpendicular to interface with other structures/cells.
- Pseudopalisading of tumour cells (around necrotic regions) is seen in glioblastoma.
{kind=link}
{kind=link}
{kind=link}
Note:
- Good set of articles: Neuropathology for radiologists (ncbi.nlm.nih.gov).
Axonal swellings
H&E:
- Eosinophilic (light pink) - ground glass-like appearance.
- Shape:
- Round if sectioned perpendicular to axis of axon.
- Bound by cell membrane.
- Large ~ typically 2-4x RBC diameter.
- Sausage-shaped if cut in along axis.
- Round if sectioned perpendicular to axis of axon.
Images:
{kind=link}
{kind=link}
IHC
- APP.
Image:
Inclusion bodies
- Negri bodies.
- Cytoplasmic inclusions; classically in Purkinje cells of the cerebellum, pyramidal cells of Ammon's horn.
- Rabies.
- Image: Negri bodies (WC/CDC).
{kind=link}
- Lewy bodies.
- Eosinophilic cytoplasmic inclusion - composed mostly of alpha-synuclein.[19]
- Image: Lewy body (WC).
{kind=link}
Table of inclusions
| Feature | Appearance | Associated disease | Comment | Image |
| Grumous bodies AKA granular bodies |
granular and eosinophilic ~50 micrometers | neurodegenerative disease, neuroaxonal dystrophies, aging | ?Comment | ?Image |
| Cowdry type 1 AKA Cowdry type A |
eosinophilic & round + halo | herpes simplex virus | can be confused with Lewy body, Marinesco body |
?Image |
| Lewy body | round cytoplasmic eosinophilic body +/- pale halo |
Parkinsons disease, dementia with Lewy bodies | morphology dependent on location in brain; +ve for alpha-synuclein, alpha-B crystallin, ubiquitin |
[1], [2] |
| Lafora body | round | myoclonic epilepsy | look like corpora amylacea; location: dentate nucleus, liver, skeletal muscle, sweat glands | ?Image |
| Lipofuscin | yellow & granular | aging | olive, dendate | ?Image |
| Negri body | small eosinophic bodies | rabies | found in hippocampal neurons and Purkinje cells | [3] |
| Hirano body | concentric calcification/rod-shaped bright eosinophilic; overlap edge of neuron | Alzheimer d., Pick d.[20] | actin crystals, may look like capillaries; location: CA1 of hippocampus | [4][21] |
| Neurofibrillary tangles | flame-shaped cytoplasmic thingy ~30 micrometers |
aging, Alzheimer's disease | seen with silver stain | Schematic[21], [5][22] |
| Granulovacuolar degeneration | cytoplasmic vacuoles 4-5 micrometers | ageing, Alzheimer's disease, Pick's disease |
main found in Ammon horn[20] | [6][22] |
| Pick bodies | round, homogenous, intracytoplasmic, ~10 micrometers | Pick's disease | pyramidal neurons, dentate granule cells (hippocampus); +ve for tau, tubulin, ubiquitin |
[7] |
| Bunina body | size of Nissl granules, eosinophilic | ALS | EM: membrane-bound bodies; ubiquitin +ve | [8] |
![[2]](http://firstaidteam.com/usmlerximages/v/USMLERxLewy+bodies.gif.html){kind=link}
![[4]](http://faculty.washington.edu/alexbert/MEDEX/Fall/adhirano.jpg){kind=link}
{kind=link}
![[5]](http://faculty.washington.edu/alexbert/MEDEX/Fall/adtangle.jpg){kind=link}
![[6]](http://faculty.washington.edu/alexbert/MEDEX/Fall/adgvd.jpg){kind=link}
![[7]](http://s212.photobucket.com/albums/cc74/cat_at_uw/Osler%20-%20Neuropath/?action=view¤t=Picks60x.jpg&mediafilter=images){kind=link}
![[8]](http://pathol.umin.ac.jp/gakubu/exam/2006jpg/19.jpg){kind=link}
Image collection: Inclusion bodies (photobucket.com).
Immunohistochemistry
General
- S-100.
- Sensitive... but non-specific, e.g. also stains melanoma.
Glial
- GFAP (glial fibrillary acidic protein) - should stain perikaryon.
Glial tumours
Standard work-up:
- GFAP.
- p53.
- Ki-67.
Neuronal
- Synaptophysin.
- Chromogranin.
Carcinoma vs. glial tumours
- AE1/AE3 often +ve in glial tumours (e.g. astrocytomas, oligodendrogliomas); CAM5.2 is usu. -ve in glial tumours.[23]
Others
- APP (amyloid precursor protein) - detects axonal swellings.
- NF (neurofilament) - detects axonal swellings.
Brain tumours
Tumours are a big part of neuropathology. The most common brain tumour is a metastasis. The most common primary tumour (in adults) is glioblastoma which has a horrible prognosis.
Non-tumour
Alcohol & CNS
Clinical
- Wernicke's encephalopathy
- Mnemonic WACO:
- Wernicke's.
- Ataxia.
- Confusion, confabulation -- Korsakoff.
- Ocular Sx (CN IV palsy).
- Cause: thiamine deficiency.
- Mnemonic WACO:
Pathology
Features:[24]
- Morel's laminar sclerosis = spongy degeneration and gliosis of the cerebral cortex[25] usu. prominent in the third layer of the cortex (outer pyramidal layer) and especially in the lateral-frontal cortex.[26]
- Central pontine myelinolysis (CPM).[27]
- Just what it sound like - myelin loss in the central pons.
- Classically associated with rapid correction of hyponatremia.[28]
- Mammillary body shrinkage.[29]
- Anterior cerebellar vermis atrophy; weak finding - as also age-related.[30]
- Vermis atrophy is also seen in schizophrenia.[31]
Marchiafava-Bignami Disease
- Rare.
- Demyelination of the corpus callosum.[26]
Wernicke's encephalopathy
General:
- Due to thiamine deficiency.
Features:
- Neurons preserved - key.
- Loss of myelin.
- Hemorrhage.
- Spongiosis.
- Reactive blood vessels.
Common non-specific findings
- Intracranial haemorrhage - due to trauma.
Meningitis
General
- Definition: inflammation of the meninges (pia mater, arachnoid membranes, dura mater).
Classic clinical presentation:
- Neck stiffness.
- Fever.
- +/-Headache.
- +/-Decreased level of consciousness.
Etiology:
- Infectious.
- Bacterial.
- Viral.
- Parasitic
- Autoimmune.
- Toxic.
Gross
Features:
- +/-Clouded appearance of the meninges.
- +/-Pus.
- +/-Petechiae.
- +/-Cerebral edema.
Image:
{kind=link}
Microscopic
Features:
- Inflammation of the meninges.
- Infectious meningitis:
- Microorganisms (bacteria, fungi).
Abscess
General
- May mimic malignancy clinically.
Microscopic
Features:
- Sheets of neutrophils surrounded by fibrosing brain.
- Fibrosing brain: pale (lighter pink than normal brain tissue), dense.
Image: Cerebral abscess (pathconsultddx.com).
Neurodegenerative diseases
This is a hueueuge topic. It is covered its own article and includes a general discussion of dementia.
Epilepsy
General
- Seizure that are "idiopathic", i.e. no brain tumour, no mass lesion, no brain injury.
- Most common form: temporal lobe epilepsy.[32]
Microscopic
Features:[33]
- Mesial temporal sclerosis = scarring of the medial temporal lobe.
- Involves: hippocampus, parahippocampal gyrus and amygdala.
- Hippocampus: CA1 and CA4 affected.
- Involves: hippocampus, parahippocampal gyrus and amygdala.
Notes:
- Changes in CA1 & CA4 of the hippocampus - DDx:
- Epilpsy.
- Dementia.
Cysts
General
- All are "benign", but some may be fatal due to spatial constraints.
List of cysts
- Colloid cyst.[34]
- Columnar epithelium.
- Arachnoid cyst - considered precursor of meningioma.
- Psammoma bodies.
- Clumps of cells.
- Whorled pattern.
- Dermoid cyst.
- Skin + adnexal structures.
- ... think of ovarian dermoid.
- Epidermoid.
- Choriod cyst.
- ?
- Neuroenteric cyst.
- Epithelial cyst.
Stroke
Gross
- Soft/mushy brain.
- Older infarcts.
- A "roof" is present - a thin submeningeal layer is preserved by the CSF.[35]
- "Roof" is absent in trauma.
- Cavity - in older infarcts.
- Multiple sclerosis does not cavitate.
- A "roof" is present - a thin submeningeal layer is preserved by the CSF.[35]
- Laminar necrosis = (thin) chalky line replaces grey mater.[36]
Hypoxic-ischemic encephalopathy
General
- Often due to cardiac arrest, i.e. global ischemia.
- Triple watershed area = parieto-occipital cortex, extrastriate occipital cortex.
Microscopic
Features:
- Hippocampal ischemic changes:
- Loss of neurons in CA1, CA3 and CA4 +/- "cavitation".
- Neuronal loss: No blue (nuclei) where there should be some.
- Cavitation: bubbles/clear spaces where there should be none.
- CA2 neurons preserved/resistant.
- Loss of neurons in CA1, CA3 and CA4 +/- "cavitation".
- Purkinje cell loss in the cerebellum and Bergmann gliosis.
- "Anoxic neurons".[38]
- Shrunken neurons with intensely eosinophilic cytoplasm and pyknotic (shrunken) nuclei.
- Pseudolaminar necrosis - (uncontrolled) cell death in the cerebral cortex in a band-like pattern,[39] with a relative preservation of cells immediately adjacent to the meninges.
Images:
- Anoxic neurons:
- Hippocampal ischemic changes:
- Pseudolaminar necrosis:
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Notes:
- Neurons of subiculum in adults - usu. normal (as they are resistant to ischemic changes).
Multiple sclerosis
General
- A bread 'n butter disease of neurology in Canada.
Radiologic/Gross
Features:[42]
- White matter lesions.
- Cerebrum (classically): periventricular distribution.
- Optic nerves (optic neuritis) - classic presentation.
Microscopic
Features:[43]
- Perivascular inflammation.
- Demyelination.
- Subcortical myelinated fibers are often spared.
Classification of MS lesions:
- Early active.
- Inactive.
- Early remyelinating.
- Late remyelinating.
Cerebral amyloid angiopathy
General
- Abbreviated CAA.
- Disease of the old.
- Strong association with lobar haemorrhage.[44]
- Cerebellar cortex.
- Cerebral cortex.
Etiology:
- Amyloid deposition in the basal lamina of smooth muscle (in the cerebellar cortex and cerebral cortex).
Microscopic
Features:
- Amorphous, acellular eosinophilic material within walls of small arteries.
- This is a high power diagnosis with congo red staining.
Special stains:
- Congo red.
- Abeta-amyloid (AKA beta-amyloid).
Notes:
- Amyloidosis is seen in all individuals with Alzheimer's disease; the amount of amyloid is what differs -- in CAA it is lots and lots.
Images:
{kind=link}
{kind=link}
Vascular malformations
Types:[45]
- Arteriovenous malformation.
- Most important clinically - highest risk of bleeding.
- Varix.
- One large (dilated) vein.
- Venous angioma.
- Many small veins.
- Caverous malformation.
- Vessels are back-to-back (no intervening parenchyma).
Also see: Sturge-Weber syndrome.
Arteriovenous malformation
General
- High risk for bleeding vis-a-vis other vascular malformations.
Gross
Features:[45]
- Classically wedge-shaped - with base toward superficial aspect and apex toward deep aspect (like pulmonary infarcts).
- Usually middle cerebral artery distribution.
Microscopic
Features:
- Large vessels with eccentric wall thickening.
- "Large" = ~ 0.5 mm (0.25-1.0 mm).
- 0.25 mm = ~ 31 RBC diameters across.
- "Large" = ~ 0.5 mm (0.25-1.0 mm).
Image: Cerebral AVM (WC).
{kind=link}
Notes:
- There is usually one feeding artery.
- The artery is often not seen.
- Arteries have a well-defined internal elastic lamina and an external elastic lamina (best seen on elastic trichrome).
- Veins do not have an external elastic lamina and have a poorly developed/thin internal elastic lamina.
Cavernous angioma
General
- Usually diagnosed by radiology.
Microscopic
Features:
- Vessels back-to-back/little intervening parenchyma.
- Muscle is absent in the vessel walls - key feature.[46]
Paediatric pathology
Joubert syndrome
- Malformation of the cerebellar vermis.[47]
Epidemiology
- Autosomal recessive - mutation in a number of genes including NPHP1, AHI1, and CEP290.[47]
Weird stuff
Acute disseminated encephalomyelitis
General
- Thought to be autoimmune; often associated with/preceded by by viral illness.[48]
- May mimic multiple sclerosis.
- Abbreviated "ADEM".
Diagnosis
- Need to r/o infection (with lumbar puncture).
- No old plaques on imaging (MRI).
Microscopic
Features:
- Spares subcortical fibres (???)
Tx
- Steroids.
- Plasmapheresis.
DDx
- Multiple sclerosis.
Cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL)
General
- Autosomal dominant disorder - as the name implies.[49]
- Causes strokes in 40-50 year-old.
- Characteristic MRI findings - present in asymptomatic individuals with mutation.
- Increased risk of myocardial infarction.[50]
Etiology
- Mutation of Notch 3 gene.[51]
- Diagnosis: proven Notch 3 mutation.
Microscopic
Features:
- +/-Subcortical infarcts.
- Patches of (non-myelinated) tissue within the white matter deep to the cortex with abundant macrophages.
- Blood vessels typically have a basophilic granularity.[52]
IHC
- Notch 3: smooth muscle and pericytes punctate +ve.[50]
Image: Notch 3 staining in CADASIL (WC).
{kind=link}
Notes:
- No cortical involvement -- this is unlike multiple sclerosis.
DDx:
- Amyloidosis.
- Binswanger's disease - multi-infarct dementia affecting subcortical white matter.
- Often diagnosed as Alzheimer's disease in the past.
Skin biopsy diagnosis
- Can be diagnosed on a skin biopsy.[53]
Electron microscopy
- Granular osmiophilic material (GOM).
See also
References
- ↑ MUN. Feb 3, 2009.
- ↑ TN2005 NS7.
- ↑ R. Kiehl. 8 November 2010.
- ↑ URL: http://www.neuropathologyweb.org/chapter1/chapter1aNeurons.html. Accessed on: 22 December 2010.
- ↑ Holland GR (1996). "Experimental trigeminal nerve injury". Crit. Rev. Oral Biol. Med. 7 (3): 237–58. PMID 8909880.
- ↑ Piercecchi-Marti MD, Pélissier-Alicot AL, Leonetti G, Tervé JP, Cianfarani F, Pellissier JF (December 2004). "Pellagra: a rare disease observed in a victim of mental and physical abuse". Am J Forensic Med Pathol 25 (4): 342–4. PMID 15577526.
- ↑ MUN. 15 November 2010.
- ↑ URL: http://www.neuropathologyweb.org/chapter1/chapter1bAstrocytes.html. Accessed on: 2 July 2010.
- ↑ Klatt, Edward C. (2006). Robbins and Cotran Atlas of Pathology (1st ed.). Saunders. pp. 202. ISBN 978-1416002741.
- ↑ 10.0 10.1 Perry, Arie; Brat, Daniel J. (2010). Practical Surgical Neuropathology: A Diagnostic Approach: A Volume in the Pattern Recognition series (1st ed.). Churchill Livingstone. pp. 18. ISBN 978-0443069826.
- ↑ URL: http://www.neuropathologyweb.org/chapter1/chapter1bAstrocytes.html. Accessed on: 7 November 2010.
- ↑ Gray, Francoise; Poirier, Jacques; De Girolami, Umberto (2003). Escourolle and Poirier's Manual of Basic Neuropathology (4th ed.). Churchill Livingstone. pp. 173. ISBN 978-0750674058.
- ↑ Weedman Molavi, Diana (2008). The Practice of Surgical Pathology: A Beginner's Guide to the Diagnostic Process (1st ed.). Springer. pp. 254. ISBN 978-0387744858.
- ↑ 14.0 14.1 14.2 14.3 14.4 14.5 Wippold FJ, Perry A (March 2006). "Neuropathology for the neuroradiologist: rosettes and pseudorosettes". AJNR Am J Neuroradiol 27 (3): 488–92. PMID 16551982.
- ↑ URL: http://moon.ouhsc.edu/kfung/IACP-OLP/APAQ-Text/N1-TU-01.htm#17. Accessed on: 3 December 2010.
- ↑ Gray, Francoise; Poirier, Jacques; De Girolami, Umberto (2003). Escourolle and Poirier's Manual of Basic Neuropathology (4th ed.). Churchill Livingstone. pp. 11. ISBN 978-0750674058.
- ↑ URL: http://frontalcortex.com/?page=oll&topic=24&qid=602. Accessed on: 3 November 2010.
- ↑ Finnie JW, Manavis J, Blumbergs PC, Kuchel TR (November 2000). "Axonal and neuronal amyloid precursor protein immunoreactivity in the brains of guinea pigs given tunicamycin". Vet. Pathol. 37 (6): 677–80. PMID 11105962. http://vet.sagepub.com/content/37/6/677.full.
- ↑ Marui W, Iseki E, Kato M, Akatsu H, Kosaka K (August 2004). "Pathological entity of dementia with Lewy bodies and its differentiation from Alzheimer's disease". Acta Neuropathol. 108 (2): 121–8. doi:10.1007/s00401-004-0869-4. PMID 15235805.
- ↑ 20.0 20.1 Gray, Francoise; Poirier, Jacques; De Girolami, Umberto (2003). Escourolle and Poirier's Manual of Basic Neuropathology (4th ed.). Churchill Livingstone. pp. 5. ISBN 978-0750674058.
- ↑ 21.0 21.1 URL: http://www.pakmed.net/academic/age/alz/alz030.htm. Accessed on: 12 November 2010.
- ↑ 22.0 22.1 URL: http://faculty.washington.edu/alexbert/MEDEX/Fall/NeuroPath_Obj.htm. Accessed on: 13 November 2010.
- ↑ Perry, Arie; Brat, Daniel J. (2010). Practical Surgical Neuropathology: A Diagnostic Approach: A Volume in the Pattern Recognition series (1st ed.). Churchill Livingstone. pp. 12. ISBN 978-0443069826.
- ↑ http://www.journals.elsevierhealth.com/periodicals/ycdip/article/S0968-6053(07)00035-X/abstract
- ↑ URL: http://content.karger.com/ProdukteDB/produkte.asp?Doi=114939. Accessed on: 22 September 2010.
- ↑ 26.0 26.1 Johkura K, Naito M, Naka T (March 2005). "Cortical involvement in Marchiafava-Bignami disease". AJNR Am J Neuroradiol 26 (3): 670–3. PMID 15760886. http://www.ajnr.org/cgi/content/full/26/3/670.
- ↑ Campbell MC (2010). "Hyponatremia and central pontine myelinolysis as a result of beer potomania: a case report". Prim Care Companion J Clin Psychiatry 12 (4). doi:10.4088/PCC.09l00936ecr. PMC 2983455. PMID 21085565. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2983455/.
- ↑ Bernsen HJ, Prick MJ (September 1999). "Improvement of central pontine myelinolysis as demonstrated by repeated magnetic resonance imaging in a patient without evidence of hyponatremia". Acta Neurol Belg 99 (3): 189–93. PMID 10544728.
- ↑ Shear PK, Sullivan EV, Lane B, Pfefferbaum A (November 1996). "Mammillary body and cerebellar shrinkage in chronic alcoholics with and without amnesia". Alcohol. Clin. Exp. Res. 20 (8): 1489-95. PMID 8947329. http://www3.interscience.wiley.com/resolve/openurl?genre=article&sid=nlm:pubmed&issn=0145-6008&date=1996&volume=20&issue=8&spage=1489.
- ↑ Torvik A (1987). "Brain lesions in alcoholics: neuropathological observations". Acta Med. Scand. Suppl. 717: 47–54. PMID 3478969.
- ↑ Sandyk R, Kay SR, Merriam AE (April 1991). "Atrophy of the cerebellar vermis: relevance to the symptoms of schizophrenia". Int. J. Neurosci. 57 (3-4): 205–12. PMID 1938163.
- ↑ URL: http://emedicine.medscape.com/article/342150-overview. Accessed on: 20 November 2010.
- ↑ MUN. 15 November 2010.
- ↑ MUN. 11 Mar 2009.
- ↑ MUN. 16 December 2009.
- ↑ URL: http://moon.ouhsc.edu/kfung/jty1/neurotest/Q03-Ans.htm. Accessed on: 26 October 2010.
- ↑ MUN. 26 November 2010.
- ↑ URL: http://www.neuropathologyweb.org/chapter2/chapter2aHIE.html. Accessed on: 12 July 2010.
- ↑ Hypoxic and Ischemic Encephalopathy. neuropathology.neoucom.edu. Accessed on: 29 December 2010.
- ↑ URL: http://moon.ouhsc.edu/kfung/iacp-olp/apaq-text/N1-MS-01-16-Ans.htm and http://moon.ouhsc.edu/kfung/iacp-olp/apaq-text/n1-ms-01.htm. Accessed on: 31 October 2010.
- ↑ URL: http://www.neuropathologyweb.org/chapter2/chapter2aHIE.html. Accessed on: 14 January 2011.
- ↑ URL: http://library.med.utah.edu/kw/ms/path.html. Accessed on: 12 July 2010.
- ↑ URL: http://library.med.utah.edu/kw/ms/path.html. Accessed on: 12 July 2010.
- ↑ Thanvi B, Robinson T (November 2006). "Sporadic cerebral amyloid angiopathy--an important cause of cerebral haemorrhage in older people". Age Ageing 35 (6): 565–71. doi:10.1093/ageing/afl108. PMID 16982664.
- ↑ 45.0 45.1 Prayson RA, Kleinschmidt-DeMasters BK (November 2006). "An algorithmic approach to the brain biopsy--part II". Arch. Pathol. Lab. Med. 130 (11): 1639–48. PMID 17076525.
- ↑ MUN. 23 November 2010.
- ↑ 47.0 47.1 http://www.ninds.nih.gov/disorders/joubert/joubert.htm
- ↑ Tenembaum S, Chitnis T, Ness J, Hahn JS (April 2007). "Acute disseminated encephalomyelitis". Neurology 68 (16 Suppl 2): S23–36. doi:10.1212/01.wnl.0000259404.51352.7f. PMID 17438235.
- ↑ Tikka, S.; Mykkänen, K.; Ruchoux, MM.; Bergholm, R.; Junna, M.; Pöyhönen, M.; Yki-Järvinen, H.; Joutel, A. et al. (Apr 2009). "Congruence between NOTCH3 mutations and GOM in 131 CADASIL patients.". Brain 132 (Pt 4): 933-9. doi:10.1093/brain/awn364. PMID 19174371.
- ↑ 50.0 50.1 Lesnik Oberstein SA, Jukema JW, Van Duinen SG, et al. (July 2003). "Myocardial infarction in cerebral autosomal dominant arteriopathy with subcortical infarcts and leukoencephalopathy (CADASIL)". Medicine (Baltimore) 82 (4): 251–6. doi:10.1097/01.md.0000085054.63483.40. PMID 12861102.
- ↑ Kalaria, RN.; Viitanen, M.; Kalimo, H.; Dichgans, M.; Tabira, T. (Nov 2004). "The pathogenesis of CADASIL: an update.". J Neurol Sci 226 (1-2): 35-9. doi:10.1016/j.jns.2004.09.008. PMID 15537516.
- ↑ Kleinschmidt-DeMasters BK, Prayson RA (November 2006). "An algorithmic approach to the brain biopsy--part I". Arch. Pathol. Lab. Med. 130 (11): 1630–8. PMID 17076524.
- ↑ Joutel A, Favrole P, Labauge P, et al. (December 2001). "Skin biopsy immunostaining with a Notch3 monoclonal antibody for CADASIL diagnosis". Lancet 358 (9298): 2049–51. doi:10.1016/S0140-6736(01)07142-2. PMID 11755616.