Difference between revisions of "Acute duodenitis"
Jump to navigation
Jump to search
(redirect w/ cat.) |
(+images, +infobox) |
||
| (One intermediate revision by the same user not shown) | |||
| Line 1: | Line 1: | ||
{{ Infobox diagnosis | |||
| Name = {{PAGENAME}} | |||
| Image = Acute duodenitis -- intermed mag.jpg | |||
| Width = | |||
| Caption = Acute duodenitis. [[H&E stain]]. | |||
| Synonyms = | |||
| Micro = [[neutrophil]]s - "found without searching", [[eosinophil]]s - "found without searching", plasma cells (increased), intraepithelial lymphocytes | |||
| Subtypes = | |||
| LMDDx = | |||
| Stains = | |||
| IHC = | |||
| EM = | |||
| Molecular = | |||
| IF = | |||
| Gross = | |||
| Grossing = | |||
| Site = [[duodenum]] | |||
| Assdx = [[Helicobacter gastritis]] | |||
| Syndromes = | |||
| Clinicalhx = | |||
| Signs = | |||
| Symptoms = | |||
| Prevalence = uncommon | |||
| Bloodwork = | |||
| Rads = | |||
| Endoscopy = erythema | |||
| Prognosis = benign | |||
| Other = | |||
| ClinDDx = | |||
| Tx = dependent on underlying cause | |||
}} | |||
'''Acute duodenitis''', abbreviated '''AD''', is an acute inflammatory process of the [[duodenum]]. It is relatively uncommon. | |||
==General== | |||
DDx: | |||
*Infection. | |||
**Helicobactor organisms in the [[stomach]]. | |||
***Helicobacter ''not'' seen unless gastric metaplasia is present.<ref>{{Cite journal | last1 = Madsen | first1 = JE. | last2 = Vetvik | first2 = K. | last3 = Aase | first3 = S. | title = Helicobacter-associated duodenitis and gastric metaplasia in duodenal ulcer patients. | journal = APMIS | volume = 99 | issue = 11 | pages = 997-1000 | month = Nov | year = 1991 | doi = | PMID = 1683540 }}</ref> | |||
*Medications ([[NSAID]]s). | |||
*[[Crohn's disease]] (usually focal/patchy). | |||
*[[Portal hypertension]] (portal hypertensive duodenopathy).<ref name=pmid12003421>{{Cite journal | last1 = Shudo | first1 = R. | last2 = Yazaki | first2 = Y. | last3 = Sakurai | first3 = S. | last4 = Uenishi | first4 = H. | last5 = Yamada | first5 = H. | last6 = Sugawara | first6 = K. | title = Duodenal erosions, a common and distinctive feature of portal hypertensive duodenopathy. | journal = Am J Gastroenterol | volume = 97 | issue = 4 | pages = 867-73 | month = Apr | year = 2002 | doi = 10.1111/j.1572-0241.2002.05602.x | PMID = 12003421 }}</ref> | |||
*[[Celiac sprue]]. | |||
==Microscopic== | |||
Features: | |||
*Intraepithelial lymphocytes. | |||
*[[Neutrophil]]s - "found without searching" - '''key feature'''. | |||
*[[Eosinophil]]s - "found without searching" - '''key feature'''. | |||
*[[Plasma cell]]s (increased). | |||
Notes: | |||
*One needs stomach concurrent biopsies to r/o Helicobactor. | |||
*Erosions make celiac sprue much less likely. | |||
*Presence of chronic inflammation useful for NSAIDs vs. Helicobacter organisms: | |||
**[[NSAID]]s not commonly assoc. with acute inflammation;<ref name=pmid8406146>{{cite journal |author=Taha AS, Dahill S, Nakshabendi I, Lee FD, Sturrock RD, Russell RI |title=Duodenal histology, ulceration, and Helicobacter pylori in the presence or absence of non-steroidal anti-inflammatory drugs |journal=Gut |volume=34 |issue=9 |pages=1162–6 |year=1993 |month=September |pmid=8406146 |pmc=1375446 |doi= |url=}}</ref> thus, without chronic inflammation NSAIDs are unlikely. | |||
***Acute NSAID-related duodenitis reported.<ref name=pmid18158085>{{cite journal |author=Hashash JG, Atweh LA, Saliba T, ''et al.'' |title=Acute NSAID-related transmural duodenitis and extensive duodenal ulceration |journal=Clin Ther |volume=29 |issue=11 |pages=2448–52 |year=2007 |month=November |pmid=18158085 |doi=10.1016/j.clinthera.2007.11.012 |url=}}</ref> | |||
===Images=== | |||
<gallery> | |||
Image: Acute duodenitis -- low mag.jpg | AD - low mag. | |||
Image: Acute duodenitis -- intermed mag.jpg | AD - intermed. mag. | |||
Image: Acute duodenitis -- high mag.jpg | AD - high mag. | |||
Image: Acute duodenitis -- very high mag.jpg | AD - very high mag. | |||
</gallery> | |||
==Sign out== | |||
<pre> | |||
DUODENUM, BIOPSY: | |||
- ACUTE DUODENITIS. | |||
</pre> | |||
===Acute on chronic duodenitis=== | |||
<pre> | |||
DUODENUM, BIOPSY: | |||
- ACUTE ON CHRONIC DUODENITIS. | |||
</pre> | |||
====Micro==== | |||
The sections show small bowel mucosa with intraepithelial neutrophils. The epithelium shows nuclear hyperchromasia, pseudostratification and nuclear enlargement; however, it matures toward the surface (reactive changes of the epithelium). | |||
Brunner's glands are found focally in the lamina propria. Gastric foveolar-type epithelium | |||
is identified. Lamina propria plasma cells are abundant. | |||
==See also== | |||
*[[Duodenum]]. | |||
*[[Chronic duodenitis]]. | |||
*[[Crohn's disease]]. | |||
==References== | |||
{{Reflist|2}} | |||
[[Category:Diagnosis]] | [[Category:Diagnosis]] | ||
[[Category:Duodenum]] | |||
Latest revision as of 00:32, 30 April 2014
Acute duodenitis, abbreviated AD, is an acute inflammatory process of the duodenum. It is relatively uncommon.
| Acute duodenitis | |
|---|---|
| Diagnosis in short | |
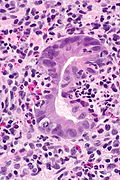
 Acute duodenitis. H&E stain. | |
|
| |
| LM | neutrophils - "found without searching", eosinophils - "found without searching", plasma cells (increased), intraepithelial lymphocytes |
| Site | duodenum |
|
| |
| Associated Dx | Helicobacter gastritis |
| Prevalence | uncommon |
| Endoscopy | erythema |
| Prognosis | benign |
| Treatment | dependent on underlying cause |
General
DDx:
- Infection.
- Medications (NSAIDs).
- Crohn's disease (usually focal/patchy).
- Portal hypertension (portal hypertensive duodenopathy).[2]
- Celiac sprue.
Microscopic
Features:
- Intraepithelial lymphocytes.
- Neutrophils - "found without searching" - key feature.
- Eosinophils - "found without searching" - key feature.
- Plasma cells (increased).
Notes:
- One needs stomach concurrent biopsies to r/o Helicobactor.
- Erosions make celiac sprue much less likely.
- Presence of chronic inflammation useful for NSAIDs vs. Helicobacter organisms:
Images

AD - low mag.

AD - intermed. mag.

AD - high mag.
AD - very high mag.



Sign out
DUODENUM, BIOPSY: - ACUTE DUODENITIS.
Acute on chronic duodenitis
DUODENUM, BIOPSY: - ACUTE ON CHRONIC DUODENITIS.
Micro
The sections show small bowel mucosa with intraepithelial neutrophils. The epithelium shows nuclear hyperchromasia, pseudostratification and nuclear enlargement; however, it matures toward the surface (reactive changes of the epithelium).
Brunner's glands are found focally in the lamina propria. Gastric foveolar-type epithelium is identified. Lamina propria plasma cells are abundant.
See also
References
- ↑ Madsen, JE.; Vetvik, K.; Aase, S. (Nov 1991). "Helicobacter-associated duodenitis and gastric metaplasia in duodenal ulcer patients.". APMIS 99 (11): 997-1000. PMID 1683540.
- ↑ Shudo, R.; Yazaki, Y.; Sakurai, S.; Uenishi, H.; Yamada, H.; Sugawara, K. (Apr 2002). "Duodenal erosions, a common and distinctive feature of portal hypertensive duodenopathy.". Am J Gastroenterol 97 (4): 867-73. doi:10.1111/j.1572-0241.2002.05602.x. PMID 12003421.
- ↑ Taha AS, Dahill S, Nakshabendi I, Lee FD, Sturrock RD, Russell RI (September 1993). "Duodenal histology, ulceration, and Helicobacter pylori in the presence or absence of non-steroidal anti-inflammatory drugs". Gut 34 (9): 1162–6. PMC 1375446. PMID 8406146. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC1375446/.
- ↑ Hashash JG, Atweh LA, Saliba T, et al. (November 2007). "Acute NSAID-related transmural duodenitis and extensive duodenal ulceration". Clin Ther 29 (11): 2448–52. doi:10.1016/j.clinthera.2007.11.012. PMID 18158085.