Difference between revisions of "Ependymoma"
(+cat.) |
Jensflorian (talk | contribs) (→Microscopic: Spinal ependymoma) |
||
| (38 intermediate revisions by 2 users not shown) | |||
| Line 1: | Line 1: | ||
# | {{ Infobox diagnosis | ||
| Name = {{PAGENAME}} | |||
| Image = Ependymoma_H%26E.jpg | |||
| Width = | |||
| Caption = Ependymoma grade II WHO. [[H&E stain]] | |||
| Synonyms = | |||
| Micro = Perivascular pseudorosettes, ependymal rosettes | |||
| Subtypes = Tanycytic, Clear cell, Papillary, Cellular | |||
| LMDDx = [[Subependymoma]], [[Glioblastoma]], [[Pilocytic astrocytoma]], [[Oligodendroglioma]] | |||
| Stains = | |||
| IHC = GFAP +ve | |||
| EM = | |||
| Molecular = | |||
| IF = | |||
| Gross = | |||
| Grossing = | |||
| Site = | |||
| Assdx = | |||
| Syndromes = | |||
| Clinicalhx = | |||
| Signs = | |||
| Symptoms = | |||
| Prevalence = | |||
| Bloodwork = | |||
| Rads = | |||
| Endoscopy = | |||
| Prognosis = intermediate to poor (WHO Grades II & III) | |||
| Other = | |||
| ClinDDx = | |||
| Tx = | |||
}} | |||
'''Ependymoma''' is a [[neuropathology tumour]]. | |||
==General== | |||
*Called the forgotten glial tumour. | |||
*Anatomic location and molecular data is essential for tumor diagnosis. | |||
Epidemiology:<ref name=Ref_PBoD8_1334>{{Ref PBoD8|1334}}</ref> | |||
*Usual site: | |||
**Adults: usually spinal cord. | |||
**Children: usually posterior fossa. | |||
*May be associated with [[neurofibromatosis type 2]]. | |||
There are currently ten main ependymal tumors:<ref name=Ref_WHOCNS_74>{{Ref WHOCNS|74}}</ref> | |||
#Supratentorial [[Subependymoma]] | |||
#Supratentorial ependymoma, ZFTA-fusion positive | |||
#Supratentorial ependymoma, YAP1-fusion positive | |||
#Posterior fossa [[Subependymoma]] | |||
#Posterior fossa ependymoma group A | |||
#Posterior fossa ependymoma group B | |||
#Spinal [[Subependymoma]] | |||
#Spinal ependymoma | |||
#Spinal ependymoma, MYCN-amplified | |||
#[[Myxopapillary ependymoma]] | |||
Ependymoma, NOS (not otherwise specified): Molecular analysis still missing. | |||
Ependymoma, NEC (not elsewhere classfied): Tumor cannot assigned to any of the defined entities. | |||
Note: Molecularly defined ependymomas can be still graded as CNS grade 2 or 3 depending on histological features. | |||
*Depreceated terminologies: | |||
**Papillary ependymoma. | |||
**Clear cell ependymoma. | |||
**Tanycytic ependymoma. | |||
**Cellular ependymoma. | |||
**Ependymoma, RELA fusion-positive.<ref>{{Cite journal | last1 = Parker | first1 = M. | last2 = Mohankumar | first2 = KM. | last3 = Punchihewa | first3 = C. | last4 = Weinlich | first4 = R. | last5 = Dalton | first5 = JD. | last6 = Li | first6 = Y. | last7 = Lee | first7 = R. | last8 = Tatevossian | first8 = RG. | last9 = Phoenix | first9 = TN. | title = C11orf95-RELA fusions drive oncogenic NF-κB signalling in ependymoma. | journal = Nature | volume = 506 | issue = 7489 | pages = 451-5 | month = Feb | year = 2014 | doi = 10.1038/nature13109 | PMID = 24553141 }}</ref><ref>{{Cite journal | last1 = Pietsch | first1 = T. | last2 = Wohlers | first2 = I. | last3 = Goschzik | first3 = T. | last4 = Dreschmann | first4 = V. | last5 = Denkhaus | first5 = D. | last6 = Dörner | first6 = E. | last7 = Rahmann | first7 = S. | last8 = Klein-Hitpass | first8 = L. | title = Supratentorial ependymomas of childhood carry C11orf95-RELA fusions leading to pathological activation of the NF-κB signaling pathway. | journal = Acta Neuropathol | volume = 127 | issue = 4 | pages = 609-11 | month = Apr | year = 2014 | doi = 10.1007/s00401-014-1264-4 | PMID = 24562983 }}</ref> This is now called Supratentorial ependymoma, ZFTA-fusion positive. | |||
**Anaplastic ependymoma. This is now called CNS grade 3 ependymoma. | |||
==Gross== | |||
*Usually discrete and enhancing. | |||
*Ventricular location, but also within the spinal cord. | |||
*Dissemination possible. | |||
*[[Myxopapillary ependymoma]] classically at [[filum terminale]]. | |||
*[[Subependymoma]] typically seen in IVth ventricle. | |||
<gallery> | |||
File:AFIP405711R-EPENDYMOMA.jpg | Radiology (AFIP) | |||
File:AFIP405713G-EPENDYMOMA.jpg | Ependymoma in the fourth ventricle (AFIP) | |||
File:Ependymoma in the fourth ventricle.jpg | Gross (AFIP) | |||
</gallery> | |||
==Microscopic== | |||
==="Classic" ependymoma=== | |||
*Come in two CNS WHO grades: 2 and 3. | |||
*Usu. sharply demarcated from surrounding brain parenchyma. | |||
Features: | |||
*Cells have a "tadpole-like" morphology. | |||
**May also be described as ''ice cream cone-shaped''.<ref>[http://www.pathology.vcu.edu/WirSelfInst/tumor-2.html http://www.pathology.vcu.edu/WirSelfInst/tumor-2.html]</ref> | |||
*'''Rosettes''' = circular nuclear free zones/cells arranged in a pseudoglandular fashion; comes in two flavours in ependymoma: | |||
**''Perivascular pseudorosettes'' = (tumour) cells arranged around a blood vessel; nuclei of cells distant from the blood vessel, i.e. rim of cytoplasm (from tumour cells) surround blood vessel (nucleus-free zone); more common than ependymal rosette... but less specific. | |||
**''Ependymal rosette'' ([[AKA]] ''true ependymal rosette'') = rosette has an empty space at the centre - '''key feature'''. | |||
*Nuclear features monotonous, i.e. "boring".<ref>MUN. 6 Oct 2009.</ref> | |||
**There is little variation in size, shape and staining. | |||
*Hyalinized vessels. | |||
*Calcification. | |||
*Rare cases with cartilagineous metaplasia.<ref>{{Cite journal | last1 = Wang | first1 = X. | last2 = Zhang | first2 = S. | last3 = Ye | first3 = Y. | last4 = Chen | first4 = Y. | last5 = Liu | first5 = X. | title = Ependymoma with cartilaginous metaplasia might have more aggressive behavior: a case report and literature review. | journal = Brain Tumor Pathol | volume = 29 | issue = 3 | pages = 172-6 | month = Jul | year = 2012 | doi = 10.1007/s10014-011-0079-4 | PMID = 22228122 }}</ref> | |||
*Branching capillaries usu. only in supratentorial ependymomas. | |||
===Supratentorial ependymoma=== | |||
*Usu. connected to the ventricles. | |||
*Mostly frontal or temporal lobe. | |||
*Approx. 1/3 of all ependymal tumours (41% in children). | |||
*Irregular CM enhancement. | |||
*YAP1-fused tumors in children oft large at time of diagnosis. | |||
*Cysts and/or calcification possible. | |||
*Sharply demarcated from adjacent brain parenchyma. | |||
*True ependymal rosettes are rare. | |||
*Occasionally branching capillary vessels. | |||
*Clear cell phenotypes more common than in other locations. | |||
*Complete surgical resection is the best predictor. | |||
*CSF spread in up to 15% of tumours. | |||
===Posterior fossa ependymoma=== | |||
*Usu. 4th ventricle, less common in CPA. | |||
*Most frequent in children. | |||
*May contain tumour nodules with increased cell density. | |||
*Micocysts, vascular hyalinization and calcification can be present. | |||
*No morphologic differences between Group A and B tumours. | |||
*Perivascular pseudorosettes almost always present. | |||
*Rare papillary or tanicytic patterns. | |||
DDx (supratentorial and posterior fossa ependymoma): | |||
*[[Subependymoma]]. | |||
*[[Glioblastoma]] (GBM). | |||
*Gliomas with BCOR internal tandem duplication. | |||
*[[Astroblastoma]], MN1-altered. | |||
**Invasive border = GBM; circumscribed border of lesion = ependymoma. | |||
*[[Oligodendroglioma]] (Clear cell ependymoma)) | |||
*CNS embryonal tumour with BCOR internal tandem duplication. | |||
===Spinal ependymoma=== | |||
*Isomorphic nuclei. | |||
*Mitotic activity usu. very low. | |||
*Calcification, hemorrhage, cystic and/or metaplastic changes may be seen. | |||
*Most tumours show CNS grade 2 histology. | |||
**CNS grade 3 tumours should be examined for MYCN amplification. | |||
*Outcome usu. good, extent of resection is prognostic. | |||
DDx (spinal ependymoma): | |||
*[[Pilocytic astrocytoma]] (Tanycytic ependymoma) | |||
*Diffuse midline glioma, H3 K27-altered | |||
*Small cell glioblastoma (MYCN-amplified spinal ependymoma) | |||
===Images=== | |||
www: | |||
*[http://www.flickr.com/photos/ckrishnan/3862487821/in/photostream Ependymoma (flickr.com)]. | |||
*[http://www.ajnr.org/cgi/content-nw/full/27/3/488/F10 Ependymoma - ependymal rosettes (ajnr.org)]. | |||
*[http://path.upmc.edu/cases/case95/micro.html Anaplastic ependymoma - case 1 (upmc.edu)]. | |||
*[http://path.upmc.edu/cases/case324.html Anaplastic ependymoma - case 2 (upmc.edu)]. | |||
<gallery> | |||
File:AFIP405736M-EPENDYMOMA.jpg | Ependymoma smear. (AFIP) | |||
File:AFIP405715M-EPENDYMOMA.jpg | Perivascular pseudorosettes in a ependymoma. (AFIP) | |||
Image:Ependymoma_intermed_mag.jpg | Ependymoma - intermed. mag. (WC) | |||
Image:Ependymoma_low_intermed_mag.jpg | Ependymoma - low mag. (WC) | |||
File:Ependymoma_H%26E.jpg | Ependymoma - high mag. (WC/Sbrandner) | |||
File:Ependymoma_true_ependymal_rosettes_and_pseudorosettes.jpg | True ependymal and pseudorosettes in a ependymoma. (WC/jensflorian) | |||
File:Ependymal_linings_ependymoma_HE.jpg | Ependymal linings in a ependymoma. (WC/jensflorian) | |||
File:Ependymoma_GFAP.jpg| GFAP IHC in a ependymoma. (WC/Sbrandner) | |||
File:EMA_ependymoma_periluminal.jpg | Periluminal EMA positivity in a ependymoma. (WC/jensflorian) | |||
File:Ependymoma_EMA.jpg | Dot-like EMA immunreactivity n a ependymoma. (WC/Marvin101) | |||
File:Tanycytic ependymoma HE.jpg | Tanycytic morphology in ependymoma must not confused with [[pilocytic astrocytoma]]. (WC/jensflorian) | |||
File:Tanicytic_ependymoma_x10.jpg | Tanycytic morphology in ependymoma - low mag. (WC/jensflorian) | |||
File:Papillary_Ependymoma.jpg | Papillary morphology in ependymoma - low mag. (WC/jensflorian) | |||
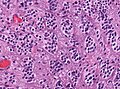
File:Papillary_ependymoma_HE_x40.jpg | Papillary morphology in ependymoma - intermed. mag. (WC/jensflorian) | |||
File:Clear_cell_ependymoma_HE.jpg | Clear cell morphology in ependymoma may mimic [[oligodendroglioma]]. (WC/jensflorian) | |||
File:HE_anaplastic_epedymomas_mitoses_pleomorphism.jpg | Brisk mitotic activity in a anaplastic ependymoma. (WC/jensflorian) | |||
File:Cartilaginous metaplasia ependymoma.jpg|Metaplastic transformation in an anaplastic ependymoma. (WC/jensflorian) | |||
File:Ependymoma_L1CAM_IHC.jpg | L1CAM immunohistochemistry indicates presence of ZFTA-fusion. | |||
File:Ependymoma_NFkappaB_IHC.jpg | Nuclear NFkappaB IHC indicates presence of ZFTA-fusion. | |||
</gallery> | |||
===Grading=== | |||
Easy: | |||
*Subependymoma = CNS WHO grade 1. | |||
*Myxopapillary ependymoma = CNS WHO grade 2. | |||
Not so easy: | |||
All other ependymomas: WHO CNS Grade 2 vs. Grade 3 depends on: | |||
*Cellular density. | |||
*Mitoses (no clear cut-off). | |||
*Necrosis (not prognostic). | |||
*Microvascular proliferation. | |||
*Poor interobserver reliability<ref>{{Cite journal | last1 = Ellison | first1 = DW. | last2 = Kocak | first2 = M. | last3 = Figarella-Branger | first3 = D. | last4 = Felice | first4 = G. | last5 = Catherine | first5 = G. | last6 = Pietsch | first6 = T. | last7 = Frappaz | first7 = D. | last8 = Massimino | first8 = M. | last9 = Grill | first9 = J. | title = Histopathological grading of pediatric ependymoma: reproducibility and clinical relevance in European trial cohorts. | journal = J Negat Results Biomed | volume = 10 | issue = | pages = 7 | month = May | year = 2011 | doi = 10.1186/1477-5751-10-7 | PMID = 21627842 }}</ref> | |||
Notes: | |||
*Many tumours fall between grade 2 and grade 3. | |||
*Rare cases with sarcomatous or cartilaginous components.<ref>{{Cite journal | last1 = Vajtai | first1 = I. | last2 = Kuhlen | first2 = D. | last3 = Kappeler | first3 = A. | last4 = Mariani | first4 = L. | last5 = Zimmermann | first5 = A. | last6 = Paulus | first6 = W. | title = Rapid spontaneous malignant progression of supratentorial tanycytic ependymoma with sarcomatous features - "Ependymosarcoma". | journal = Pathol Res Pract | volume = 206 | issue = 7 | pages = 493-8 | month = Jul | year = 2010 | doi = 10.1016/j.prp.2009.07.013 | PMID = 19853384 }}</ref><ref>{{Cite journal | last1 = Boukas | first1 = A. | last2 = Joshi | first2 = A. | last3 = Jenkins | first3 = A. | last4 = Holliman | first4 = D. | title = Extensive cartilaginous metaplasia of recurrent posterior fossa ependymoma: case report and review of the literature. | journal = Pediatr Neurosurg | volume = 49 | issue = 2 | pages = 93-8 | month = | year = 2013 | doi = 10.1159/000356931 | PMID = 24401698 }}</ref> | |||
==IHC== | |||
*Reticulin-ve. | |||
*GFAP+ve. | |||
*MIB1 (usu low). | |||
*[[IDH-1]]-ve. | |||
*EMA (dots and rings).<ref>{{Cite journal | last1 = Hasselblatt | first1 = M. | last2 = Paulus | first2 = W. | title = Sensitivity and specificity of epithelial membrane antigen staining patterns in ependymomas. | journal = Acta Neuropathol | volume = 106 | issue = 4 | pages = 385-8 | month = Oct | year = 2003 | doi = 10.1007/s00401-003-0752-8 | PMID = 12898159 }}</ref> | |||
**Widespread and strong EMA expression is indicative of YAP1-fused ependymoma. | |||
*Olig2-ve.<ref>{{Cite journal | last1 = Švajdler | first1 = M. | last2 = Rychlý | first2 = B. | last3 = Mezencev | first3 = R. | last4 = Fröhlichová | first4 = L. | last5 = Bednárová | first5 = A. | last6 = Pataky | first6 = F. | last7 = Daum | first7 = O. | title = SOX10 and Olig2 as negative markers for the diagnosis of ependymomas: An immunohistochemical study of 98 glial tumors. | journal = Histol Histopathol | volume = 31 | issue = 1 | pages = 95-102 | month = Jan | year = 2016 | doi = 10.14670/HH-11-654 | PMID = 26287936 }}</ref> | |||
*H3K27me3 nuclear loss in Posterior fossa group A ependymoma (nuclear loss is diagnostic).<ref>{{Cite journal | last1 = Panwalkar | first1 = P. | last2 = Clark | first2 = J. | last3 = Ramaswamy | first3 = V. | last4 = Hawes | first4 = D. | last5 = Yang | first5 = F. | last6 = Dunham | first6 = C. | last7 = Yip | first7 = S. | last8 = Hukin | first8 = J. | last9 = Sun | first9 = Y. | title = Immunohistochemical analysis of H3K27me3 demonstrates global reduction in group-A childhood posterior fossa ependymoma and is a powerful predictor of outcome. | journal = Acta Neuropathol | volume = | issue = | pages = | month = Jul | year = 2017 | doi = 10.1007/s00401-017-1752-4 | PMID = 28733933 }}</ref> | |||
*L1CAM in supratentorial tumors (expression indicates ZFTA fusion).<ref>{{Cite journal | last1 = Parker | first1 = M. | last2 = Mohankumar | first2 = KM. | last3 = Punchihewa | first3 = C. | last4 = Weinlich | first4 = R. | last5 = Dalton | first5 = JD. | last6 = Li | first6 = Y. | last7 = Lee | first7 = R. | last8 = Tatevossian | first8 = RG. | last9 = Phoenix | first9 = TN. | title = C11orf95-RELA fusions drive oncogenic NF-κB signalling in ependymoma. | journal = Nature | volume = 506 | issue = 7489 | pages = 451-5 | month = Feb | year = 2014 | doi = 10.1038/nature13109 | PMID = 24553141 }}</ref> | |||
*p65 nuclear +ve in ZFTA-fused ependymoma. | |||
==Molecular== | |||
'''Supratentorial Ependymoma''' | |||
*SE, ZFTA-fusion positive: Adults and children (up to 80% of cases).<ref>{{Cite journal | last1 = Parker | first1 = M. | last2 = Mohankumar | first2 = KM. | last3 = Punchihewa | first3 = C. | last4 = Weinlich | first4 = R. | last5 = Dalton | first5 = JD. | last6 = Li | first6 = Y. | last7 = Lee | first7 = R. | last8 = Tatevossian | first8 = RG. | last9 = Phoenix | first9 = TN. | title = C11orf95-RELA fusions drive oncogenic NF-κB signalling in ependymoma. | journal = Nature | volume = 506 | issue = 7489 | pages = 451-5 | month = Feb | year = 2014 | doi = 10.1038/nature13109 | PMID = 24553141 }}</ref> | |||
**ZFTA-RELA fusion most common alteration. | |||
**Chromothripsis. | |||
**EPHB2 amplifications and CDKN2A deletions in a subset of these tumors<ref>{{Cite journal | last1 = Philip-Hollingsworth | first1 = S. | last2 = Hollingsworth | first2 = RI. | last3 = Dazzo | first3 = FB. | title = Host-range related structural features of the acidic extracellular polysaccharides of Rhizobium trifolii and Rhizobium leguminosarum. | journal = J Biol Chem | volume = 264 | issue = 3 | pages = 1461-6 | month = Jan | year = 1989 | doi = | PMID = 2912966 }}</ref> | |||
*SE, YAP-fusion positive. | |||
**Restricted to children (6-7% of all supratentorial ependymomas). | |||
**YAP-MAMLD fusion most common alteration. | |||
'''Posterior fossa Ependymoma''' | |||
Two distinct molecular subgroups exist in the posterior fossa:<ref>{{Cite journal | last1 = Witt | first1 = H. | last2 = Mack | first2 = SC. | last3 = Ryzhova | first3 = M. | last4 = Bender | first4 = S. | last5 = Sill | first5 = M. | last6 = Isserlin | first6 = R. | last7 = Benner | first7 = A. | last8 = Hielscher | first8 = T. | last9 = Milde | first9 = T. | title = Delineation of two clinically and molecularly distinct subgroups of posterior fossa ependymoma. | journal = Cancer Cell | volume = 20 | issue = 2 | pages = 143-57 | month = Aug | year = 2011 | doi = 10.1016/j.ccr.2011.07.007 | PMID = 21840481 }}</ref> | |||
* Group A ependymomas: | |||
**typically found in children. | |||
**laterally. | |||
**relatively unfavorable clinical outcome. | |||
**CpG island methylator phenotype.<ref>{{Cite journal | last1 = Mack | first1 = SC. | last2 = Witt | first2 = H. | last3 = Piro | first3 = RM. | last4 = Gu | first4 = L. | last5 = Zuyderduyn | first5 = S. | last6 = Stütz | first6 = AM. | last7 = Wang | first7 = X. | last8 = Gallo | first8 = M. | last9 = Garzia | first9 = L. | title = Epigenomic alterations define lethal CIMP-positive ependymomas of infancy. | journal = Nature | volume = 506 | issue = 7489 | pages = 445-50 | month = Feb | year = 2014 | doi = 10.1038/nature13108 | PMID = 24553142 }}</ref> | |||
**Loss of H3K27me.<ref>{{Cite journal | last1 = Panwalkar | first1 = P. | last2 = Clark | first2 = J. | last3 = Ramaswamy | first3 = V. | last4 = Hawes | first4 = D. | last5 = Yang | first5 = F. | last6 = Dunham | first6 = C. | last7 = Yip | first7 = S. | last8 = Hukin | first8 = J. | last9 = Sun | first9 = Y. | title = Immunohistochemical analysis of H3K27me3 demonstrates global reduction in group-A childhood posterior fossa ependymoma and is a powerful predictor of outcome. | journal = Acta Neuropathol | volume = | issue = | pages = | month = Jul | year = 2017 | doi = 10.1007/s00401-017-1752-4 | PMID = 28733933 }}</ref> | |||
* Group B ependymomas: | |||
**typically adults. | |||
**midline. | |||
**relatively favorable clinical outcomes. | |||
**gene expression profiles similar to that of spinal cord ependymomas. | |||
**increased Chromosomal 1q gains. <ref>{{Cite journal | last1 = Korshunov | first1 = A. | last2 = Witt | first2 = H. | last3 = Hielscher | first3 = T. | last4 = Benner | first4 = A. | last5 = Remke | first5 = M. | last6 = Ryzhova | first6 = M. | last7 = Milde | first7 = T. | last8 = Bender | first8 = S. | last9 = Wittmann | first9 = A. | title = Molecular staging of intracranial ependymoma in children and adults. | journal = J Clin Oncol | volume = 28 | issue = 19 | pages = 3182-90 | month = Jul | year = 2010 | doi = 10.1200/JCO.2009.27.3359 | PMID = 20516456 }}</ref> | |||
==See also== | |||
*[[Subependymoma]]. | |||
*[[Myxopapillary ependymoma]]. | |||
*[[Neuropathology tumours]]. | |||
==References== | |||
{{Reflist|1}} | |||
[[Category:Diagnosis]] | [[Category:Diagnosis]] | ||
[[Category:Neuropathology tumours]] | |||
Latest revision as of 13:20, 19 September 2022
Ependymoma is a neuropathology tumour.
| Ependymoma | |
|---|---|
| Diagnosis in short | |
|
Template:Px Ependymoma grade II WHO. H&E stain | |
|
| |
| LM | Perivascular pseudorosettes, ependymal rosettes |
| Subtypes | Tanycytic, Clear cell, Papillary, Cellular |
| LM DDx | Subependymoma, Glioblastoma, Pilocytic astrocytoma, Oligodendroglioma |
| IHC | GFAP +ve |
| Prognosis | intermediate to poor (WHO Grades II & III) |
General
- Called the forgotten glial tumour.
- Anatomic location and molecular data is essential for tumor diagnosis.
Epidemiology:[1]
- Usual site:
- Adults: usually spinal cord.
- Children: usually posterior fossa.
- May be associated with neurofibromatosis type 2.
There are currently ten main ependymal tumors:[2]
- Supratentorial Subependymoma
- Supratentorial ependymoma, ZFTA-fusion positive
- Supratentorial ependymoma, YAP1-fusion positive
- Posterior fossa Subependymoma
- Posterior fossa ependymoma group A
- Posterior fossa ependymoma group B
- Spinal Subependymoma
- Spinal ependymoma
- Spinal ependymoma, MYCN-amplified
- Myxopapillary ependymoma
Ependymoma, NOS (not otherwise specified): Molecular analysis still missing. Ependymoma, NEC (not elsewhere classfied): Tumor cannot assigned to any of the defined entities.
Note: Molecularly defined ependymomas can be still graded as CNS grade 2 or 3 depending on histological features.
Gross
- Usually discrete and enhancing.
- Ventricular location, but also within the spinal cord.
- Dissemination possible.
- Myxopapillary ependymoma classically at filum terminale.
- Subependymoma typically seen in IVth ventricle.
Radiology (AFIP)

Ependymoma in the fourth ventricle (AFIP)
- Ependymoma in the fourth ventricle.jpg
Gross (AFIP)

Microscopic
"Classic" ependymoma
- Come in two CNS WHO grades: 2 and 3.
- Usu. sharply demarcated from surrounding brain parenchyma.
Features:
- Cells have a "tadpole-like" morphology.
- May also be described as ice cream cone-shaped.[5]
- Rosettes = circular nuclear free zones/cells arranged in a pseudoglandular fashion; comes in two flavours in ependymoma:
- Perivascular pseudorosettes = (tumour) cells arranged around a blood vessel; nuclei of cells distant from the blood vessel, i.e. rim of cytoplasm (from tumour cells) surround blood vessel (nucleus-free zone); more common than ependymal rosette... but less specific.
- Ependymal rosette (AKA true ependymal rosette) = rosette has an empty space at the centre - key feature.
- Nuclear features monotonous, i.e. "boring".[6]
- There is little variation in size, shape and staining.
- Hyalinized vessels.
- Calcification.
- Rare cases with cartilagineous metaplasia.[7]
- Branching capillaries usu. only in supratentorial ependymomas.
Supratentorial ependymoma
- Usu. connected to the ventricles.
- Mostly frontal or temporal lobe.
- Approx. 1/3 of all ependymal tumours (41% in children).
- Irregular CM enhancement.
- YAP1-fused tumors in children oft large at time of diagnosis.
- Cysts and/or calcification possible.
- Sharply demarcated from adjacent brain parenchyma.
- True ependymal rosettes are rare.
- Occasionally branching capillary vessels.
- Clear cell phenotypes more common than in other locations.
- Complete surgical resection is the best predictor.
- CSF spread in up to 15% of tumours.
Posterior fossa ependymoma
- Usu. 4th ventricle, less common in CPA.
- Most frequent in children.
- May contain tumour nodules with increased cell density.
- Micocysts, vascular hyalinization and calcification can be present.
- No morphologic differences between Group A and B tumours.
- Perivascular pseudorosettes almost always present.
- Rare papillary or tanicytic patterns.
DDx (supratentorial and posterior fossa ependymoma):
- Subependymoma.
- Glioblastoma (GBM).
- Gliomas with BCOR internal tandem duplication.
- Astroblastoma, MN1-altered.
- Invasive border = GBM; circumscribed border of lesion = ependymoma.
- Oligodendroglioma (Clear cell ependymoma))
- CNS embryonal tumour with BCOR internal tandem duplication.
Spinal ependymoma
- Isomorphic nuclei.
- Mitotic activity usu. very low.
- Calcification, hemorrhage, cystic and/or metaplastic changes may be seen.
- Most tumours show CNS grade 2 histology.
- CNS grade 3 tumours should be examined for MYCN amplification.
- Outcome usu. good, extent of resection is prognostic.
DDx (spinal ependymoma):
- Pilocytic astrocytoma (Tanycytic ependymoma)
- Diffuse midline glioma, H3 K27-altered
- Small cell glioblastoma (MYCN-amplified spinal ependymoma)
Images
www:
- Ependymoma (flickr.com).
- Ependymoma - ependymal rosettes (ajnr.org).
- Anaplastic ependymoma - case 1 (upmc.edu).
- Anaplastic ependymoma - case 2 (upmc.edu).
- AFIP405736M-EPENDYMOMA.jpg
Ependymoma smear. (AFIP)
Perivascular pseudorosettes in a ependymoma. (AFIP)
- Ependymoma intermed mag.jpg
Ependymoma - intermed. mag. (WC)
- Ependymoma low intermed mag.jpg
Ependymoma - low mag. (WC)
- Ependymoma H&E.jpg
Ependymoma - high mag. (WC/Sbrandner)
True ependymal and pseudorosettes in a ependymoma. (WC/jensflorian)
- Ependymal linings ependymoma HE.jpg
Ependymal linings in a ependymoma. (WC/jensflorian)
GFAP IHC in a ependymoma. (WC/Sbrandner)
Periluminal EMA positivity in a ependymoma. (WC/jensflorian)
Dot-like EMA immunreactivity n a ependymoma. (WC/Marvin101)
- Tanycytic ependymoma HE.jpg
Tanycytic morphology in ependymoma must not confused with pilocytic astrocytoma. (WC/jensflorian)
Tanycytic morphology in ependymoma - low mag. (WC/jensflorian)
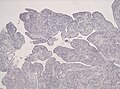
Papillary morphology in ependymoma - low mag. (WC/jensflorian)
Papillary morphology in ependymoma - intermed. mag. (WC/jensflorian)
Clear cell morphology in ependymoma may mimic oligodendroglioma. (WC/jensflorian)
Brisk mitotic activity in a anaplastic ependymoma. (WC/jensflorian)
Metaplastic transformation in an anaplastic ependymoma. (WC/jensflorian)

L1CAM immunohistochemistry indicates presence of ZFTA-fusion.
- Ependymoma NFkappaB IHC.jpg
Nuclear NFkappaB IHC indicates presence of ZFTA-fusion.


{kind=link}
Grading
Easy:
- Subependymoma = CNS WHO grade 1.
- Myxopapillary ependymoma = CNS WHO grade 2.
Not so easy: All other ependymomas: WHO CNS Grade 2 vs. Grade 3 depends on:
- Cellular density.
- Mitoses (no clear cut-off).
- Necrosis (not prognostic).
- Microvascular proliferation.
- Poor interobserver reliability[8]
Notes:
IHC
- Reticulin-ve.
- GFAP+ve.
- MIB1 (usu low).
- IDH-1-ve.
- EMA (dots and rings).[11]
- Widespread and strong EMA expression is indicative of YAP1-fused ependymoma.
- Olig2-ve.[12]
- H3K27me3 nuclear loss in Posterior fossa group A ependymoma (nuclear loss is diagnostic).[13]
- L1CAM in supratentorial tumors (expression indicates ZFTA fusion).[14]
- p65 nuclear +ve in ZFTA-fused ependymoma.
Molecular
Supratentorial Ependymoma
- SE, ZFTA-fusion positive: Adults and children (up to 80% of cases).[15]
- ZFTA-RELA fusion most common alteration.
- Chromothripsis.
- EPHB2 amplifications and CDKN2A deletions in a subset of these tumors[16]
- SE, YAP-fusion positive.
- Restricted to children (6-7% of all supratentorial ependymomas).
- YAP-MAMLD fusion most common alteration.
Posterior fossa Ependymoma Two distinct molecular subgroups exist in the posterior fossa:[17]
- Group A ependymomas:
- Group B ependymomas:
- typically adults.
- midline.
- relatively favorable clinical outcomes.
- gene expression profiles similar to that of spinal cord ependymomas.
- increased Chromosomal 1q gains. [20]
See also
References
- ↑ Kumar, Vinay; Abbas, Abul K.; Fausto, Nelson; Aster, Jon (2009). Robbins and Cotran pathologic basis of disease (8th ed.). Elsevier Saunders. pp. 1334. ISBN 978-1416031215.
- ↑ The International Agency for Research on Cancer (Editors: Louis, D.N.; Ohgaki, H.; Wiestler, O.D.; Cavenee, W.K.) (2007). Pathology and Genetics of Tumours of Tumors of the Central Nervous System (IARC WHO Classification of Tumours) (4th ed.). Lyon: World Health Organization. pp. 74. doi:10.1007/s00401-007-0243-4. ISBN 978-9283224303.
- ↑ Parker, M.; Mohankumar, KM.; Punchihewa, C.; Weinlich, R.; Dalton, JD.; Li, Y.; Lee, R.; Tatevossian, RG. et al. (Feb 2014). "C11orf95-RELA fusions drive oncogenic NF-κB signalling in ependymoma.". Nature 506 (7489): 451-5. doi:10.1038/nature13109. PMID 24553141.
- ↑ Pietsch, T.; Wohlers, I.; Goschzik, T.; Dreschmann, V.; Denkhaus, D.; Dörner, E.; Rahmann, S.; Klein-Hitpass, L. (Apr 2014). "Supratentorial ependymomas of childhood carry C11orf95-RELA fusions leading to pathological activation of the NF-κB signaling pathway.". Acta Neuropathol 127 (4): 609-11. doi:10.1007/s00401-014-1264-4. PMID 24562983.
- ↑ http://www.pathology.vcu.edu/WirSelfInst/tumor-2.html
- ↑ MUN. 6 Oct 2009.
- ↑ Wang, X.; Zhang, S.; Ye, Y.; Chen, Y.; Liu, X. (Jul 2012). "Ependymoma with cartilaginous metaplasia might have more aggressive behavior: a case report and literature review.". Brain Tumor Pathol 29 (3): 172-6. doi:10.1007/s10014-011-0079-4. PMID 22228122.
- ↑ Ellison, DW.; Kocak, M.; Figarella-Branger, D.; Felice, G.; Catherine, G.; Pietsch, T.; Frappaz, D.; Massimino, M. et al. (May 2011). "Histopathological grading of pediatric ependymoma: reproducibility and clinical relevance in European trial cohorts.". J Negat Results Biomed 10: 7. doi:10.1186/1477-5751-10-7. PMID 21627842.
- ↑ Vajtai, I.; Kuhlen, D.; Kappeler, A.; Mariani, L.; Zimmermann, A.; Paulus, W. (Jul 2010). "Rapid spontaneous malignant progression of supratentorial tanycytic ependymoma with sarcomatous features - "Ependymosarcoma".". Pathol Res Pract 206 (7): 493-8. doi:10.1016/j.prp.2009.07.013. PMID 19853384.
- ↑ Boukas, A.; Joshi, A.; Jenkins, A.; Holliman, D. (2013). "Extensive cartilaginous metaplasia of recurrent posterior fossa ependymoma: case report and review of the literature.". Pediatr Neurosurg 49 (2): 93-8. doi:10.1159/000356931. PMID 24401698.
- ↑ Hasselblatt, M.; Paulus, W. (Oct 2003). "Sensitivity and specificity of epithelial membrane antigen staining patterns in ependymomas.". Acta Neuropathol 106 (4): 385-8. doi:10.1007/s00401-003-0752-8. PMID 12898159.
- ↑ Švajdler, M.; Rychlý, B.; Mezencev, R.; Fröhlichová, L.; Bednárová, A.; Pataky, F.; Daum, O. (Jan 2016). "SOX10 and Olig2 as negative markers for the diagnosis of ependymomas: An immunohistochemical study of 98 glial tumors.". Histol Histopathol 31 (1): 95-102. doi:10.14670/HH-11-654. PMID 26287936.
- ↑ Panwalkar, P.; Clark, J.; Ramaswamy, V.; Hawes, D.; Yang, F.; Dunham, C.; Yip, S.; Hukin, J. et al. (Jul 2017). "Immunohistochemical analysis of H3K27me3 demonstrates global reduction in group-A childhood posterior fossa ependymoma and is a powerful predictor of outcome.". Acta Neuropathol. doi:10.1007/s00401-017-1752-4. PMID 28733933.
- ↑ Parker, M.; Mohankumar, KM.; Punchihewa, C.; Weinlich, R.; Dalton, JD.; Li, Y.; Lee, R.; Tatevossian, RG. et al. (Feb 2014). "C11orf95-RELA fusions drive oncogenic NF-κB signalling in ependymoma.". Nature 506 (7489): 451-5. doi:10.1038/nature13109. PMID 24553141.
- ↑ Parker, M.; Mohankumar, KM.; Punchihewa, C.; Weinlich, R.; Dalton, JD.; Li, Y.; Lee, R.; Tatevossian, RG. et al. (Feb 2014). "C11orf95-RELA fusions drive oncogenic NF-κB signalling in ependymoma.". Nature 506 (7489): 451-5. doi:10.1038/nature13109. PMID 24553141.
- ↑ Philip-Hollingsworth, S.; Hollingsworth, RI.; Dazzo, FB. (Jan 1989). "Host-range related structural features of the acidic extracellular polysaccharides of Rhizobium trifolii and Rhizobium leguminosarum.". J Biol Chem 264 (3): 1461-6. PMID 2912966.
- ↑ Witt, H.; Mack, SC.; Ryzhova, M.; Bender, S.; Sill, M.; Isserlin, R.; Benner, A.; Hielscher, T. et al. (Aug 2011). "Delineation of two clinically and molecularly distinct subgroups of posterior fossa ependymoma.". Cancer Cell 20 (2): 143-57. doi:10.1016/j.ccr.2011.07.007. PMID 21840481.
- ↑ Mack, SC.; Witt, H.; Piro, RM.; Gu, L.; Zuyderduyn, S.; Stütz, AM.; Wang, X.; Gallo, M. et al. (Feb 2014). "Epigenomic alterations define lethal CIMP-positive ependymomas of infancy.". Nature 506 (7489): 445-50. doi:10.1038/nature13108. PMID 24553142.
- ↑ Panwalkar, P.; Clark, J.; Ramaswamy, V.; Hawes, D.; Yang, F.; Dunham, C.; Yip, S.; Hukin, J. et al. (Jul 2017). "Immunohistochemical analysis of H3K27me3 demonstrates global reduction in group-A childhood posterior fossa ependymoma and is a powerful predictor of outcome.". Acta Neuropathol. doi:10.1007/s00401-017-1752-4. PMID 28733933.
- ↑ Korshunov, A.; Witt, H.; Hielscher, T.; Benner, A.; Remke, M.; Ryzhova, M.; Milde, T.; Bender, S. et al. (Jul 2010). "Molecular staging of intracranial ependymoma in children and adults.". J Clin Oncol 28 (19): 3182-90. doi:10.1200/JCO.2009.27.3359. PMID 20516456.