Difference between revisions of "Sebaceous carcinoma"
(redirect) |
|||
| (10 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
{{ Infobox diagnosis | |||
| Name = {{PAGENAME}} | |||
| Image = Sebaceous_carcinoma_-_high_mag.jpg | |||
| Width = | |||
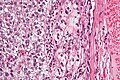
| Caption = Sebaceous carcinoma. [[H&E stain]]. | |||
| Micro = sebaceous differentiation (may be a minor component): sebocytes (abundant pale fluffy cytoplasm with vacuolization); basaloid cells (often dominant); | |||
nodular or diffuse growth pattern surrounded by a dense fibrous stroma; infiltrative border; +/-nuclear atypia, +/-squamous differentiation, +/-foreign body-type [[giant cells]] | |||
| Subtypes = | |||
| LMDDx = [[sebaceous adenoma]], [[squamous cell carcinoma]] (clear cell variant), [[malignant melanoma]], [[extramammary Paget disease]], [[trichoblastoma]],[[basal cell carcinoma]], [[sweat gland carcinoma]] | |||
| Stains = | |||
| IHC = EMA +ve (only sebaceous component), CEA -ve | |||
| EM = | |||
| Molecular = | |||
| IF = | |||
| Gross = yellow or red (ulcerated) nodule | |||
| Grossing = | |||
| Site = [[skin]] - usu. [[head and neck pathology|head and neck]], [[salivary gland]] | |||
| Assdx = | |||
| Syndromes = [[Muir-Torre syndrome]] | |||
| Clinicalhx = | |||
| Signs = | |||
| Symptoms = | |||
| Prevalence = uncommon | |||
| Bloodwork = | |||
| Rads = | |||
| Endoscopy = | |||
| Prognosis = | |||
| Other = | |||
| ClinDDx = | |||
}} | |||
'''Sebaceous carcinoma''', also known as '''sebaceous cell carcinoma''', is an uncommon [[dermatologic neoplasms|skin tumour]]. | |||
==General== | |||
*Malignant. | |||
*May arise in a [[salivary gland]].<ref name=Warman/> | |||
*Can be part of [[Muir-Torre syndrome]]. | |||
Notes: | |||
*Sebaceous lesions (from benign to malignant): [[sebaceous hyperplasia]], [[sebaceous adenoma]], sebaceoma, sebaceous carcinoma. | |||
==Gross== | |||
Features:<ref name=Ref_Derm431>{{Ref Derm|431}}</ref> | |||
*Classically [[head and neck pathology|head and neck]] tumour. | |||
*Yellow or red (ulcerated) nodule. | |||
==Microscopic== | |||
Features:<ref name=Ref_Derm431-2>{{Ref Derm|431-2}}</ref> | |||
*Sebaceous differentiation - may be a minor component - '''key feature'''. | |||
**Sebocytes = abundant pale fluffy cytoplasm with vacuolization. | |||
*Basaloid cells - often dominant. | |||
**May lead to confusion with basaloid tumours. | |||
*Nodular or diffuse growth pattern surrounded by a dense fibrous stroma. | |||
*Infiltrative border - '''important'''. | |||
**The key difference with [[sebaceous adenoma]] in cases where there isn't significant nuclear atypia. | |||
*+/-Nuclear atypia. | |||
*+/-Squamous differentiation. | |||
*+/-Foreign body-type [[giant cells]]. | |||
DDx: | |||
*[[Sebaceous adenoma]] - non-infiltrative border. | |||
*[[Squamous cell carcinoma]], clear cell variant. | |||
*[[Malignant melanoma]]. | |||
*[[Extramammary Paget disease]]. | |||
*[[Trichoblastoma]]. | |||
*[[Basal cell carcinoma]]. | |||
*[[Sweat gland carcinoma]]. | |||
===Images=== | |||
<gallery> | |||
Image:Sebaceous_carcinoma_-_intermed_mag.jpg | Sebaceous carcinoma - intermed. mag. (WC/Nephron) | |||
Image:Sebaceous_carcinoma_-_high_mag.jpg | Sebaceous carcinoma - high mag. (WC/Nephron) | |||
Image:Sebaceous_carcinoma_-_very_high_mag.jpg | Sebaceous carcinoma - very high mag. (WC/Nephron) | |||
</gallery> | |||
www: | |||
*[http://www.ispub.com/journal/the-internet-journal-of-otorhinolaryngology/volume-9-number-2/sebaceous-adenocarcinoma-of-the-parotid-gland-a-case-report-and-literature-review.article-g01.fs.jpg Sebaceous carcinoma (ispub.com)].<ref name=Warman>URL: [http://www.ispub.com/journal/the_internet_journal_of_otorhinolaryngology/volume_9_number_2_11/article/sebaceous_adenocarcinoma_of_the_parotid_gland_a_case_report_and_literature_review.html http://www.ispub.com/journal/the_internet_journal_of_otorhinolaryngology/volume_9_number_2_11/article/sebaceous_adenocarcinoma_of_the_parotid_gland_a_case_report_and_literature_review.html]. Accessed on: 8 September 2011.</ref> | |||
===Grading=== | |||
Three tier system:<ref name=Ref_Derm431-2>{{Ref Derm|431-2}}</ref> | |||
*Well-differentiated - sebocytes predominant. | |||
*Moderately differentiated - sebocytes are easily recognized but a minor component. | |||
*Poorly differentiated - sebocytes are rare. | |||
==IHC== | |||
Features:<ref name=Ref_Derm431-2>{{Ref Derm|431-2}}</ref> | |||
*CK7 +ve<ref name=pmid21592202>{{Cite journal | last1 = Ansai | first1 = S. | last2 = Arase | first2 = S. | last3 = Kawana | first3 = S. | last4 = Kimura | first4 = T. | title = Immunohistochemical findings of sebaceous carcinoma and sebaceoma: retrieval of cytokeratin expression by a panel of anti-cytokeratin monoclonal antibodies. | journal = J Dermatol | volume = 38 | issue = 10 | pages = 951-8 | month = Oct | year = 2011 | doi = 10.1111/j.1346-8138.2011.01274.x | PMID = 21592202 }}</ref> - often weak. | |||
*EMA +ve -- only sebaceous component.<ref name=pmid10369589/> | |||
*CEA -ve. | |||
**Positive in [[extramammary Paget disease]], sweat duct tumours. | |||
Images: | |||
*[http://archopht.jamanetwork.com/data/journals/ophth/9858/m_ecs8482f1.png Sebaceous carcinoma - EMA, AE1/AE3, CAM5.2 (jamanetwork.com)].<ref name=pmid10369589>{{Cite journal | last1 = Sinard | first1 = JH. | title = Immunohistochemical distinction of ocular sebaceous carcinoma from basal cell and squamous cell carcinoma. | journal = Arch Ophthalmol | volume = 117 | issue = 6 | pages = 776-83 | month = Jun | year = 1999 | doi = | PMID = 10369589 }}</ref> | |||
===Sebaceous carcinoma versus squamous cell carcinoma=== | |||
*CK7 +ve. | |||
**Useful if positive: 24 of 27 sebaceous carcinomas +ve; only 2 of 22 squamous cell carcinomas +ve.<ref name=pmid26485238>{{cite journal |authors=Plaza JA, Mackinnon A, Carrillo L, Prieto VG, Sangueza M, Suster S |title=Role of immunohistochemistry in the diagnosis of sebaceous carcinoma: a clinicopathologic and immunohistochemical study |journal=Am J Dermatopathol |volume=37 |issue=11 |pages=809–21 |date=November 2015 |pmid=26485238 |doi=10.1097/DAD.0000000000000255 |url=}}</ref> | |||
*Ber-EP4 -ve/+ve. | |||
**Useful if positive: 7 of 27 sebaceous carcinomas +ve; 0 of 22 squamous cell carcinomas +ve.<ref name=pmid26485238/> | |||
*EMA +ve. | |||
**Useful if negative: 27 of 27 sebaceous carcinoma +ve; 16 of 22 squamous cell carcinoma +ve.<ref name=pmid26485238/> | |||
==Sign out== | |||
<pre> | |||
SKIN LESION, NOSE, BIOPSY: | |||
- SEBACEOUS CARCINOMA, WELL-DIFFERENTIATED, COMPLETELY EXCISED IN THE PLANE OF SECTION. | |||
COMMENT: | |||
EMA staining marks the sebocytes. The lesion is negative for Ber-EP4. | |||
Sebaceous carcinoma may be seen in the context of Muir-Torre syndrome. | |||
</pre> | |||
===Micro=== | |||
====Well differentiated==== | |||
The sections show well-circumscribed dermal nests of basaloid cells with peripheral palisading, | |||
surrounded by a dense fibrous stroma. The basaloid cells have distinct nucleoli. Focally, the | |||
basaloid nests contain small clusters of cells with abundant pale, vacuolated, fluffy-appearing | |||
cytoplasm (sebocytes). Mitotic activity is minimal. | |||
There is no artefactual clefting between the stroma and basaloid cell nests. The epidermis | |||
matures to the surface and does not have basal atypia. | |||
The lesion is completely excised in the plane of section. | |||
====Poor differentiated==== | |||
The sections show well-circumscribed dermal nests of basaloid cells with peripheral | |||
palisading, surrounded by a dense fibrous stroma, that extend from the skin surface almost | |||
to the adipose tissue. The basaloid cells have moderate nuclear atypia with occasional monstrous cells. Mitotic activity is abundant and atypical mitoses are present. The nests contain rare cells with pale, fluffy-appearing cytoplasm, suggestive of sebocytes. | |||
==See also== | |||
*[[Dermatologic neoplasms]]. | |||
==References== | |||
{{Reflist|2}} | |||
[[Category:Dermatologic neoplasms]] | |||
[[Category:Diagnosis]] | |||
Latest revision as of 21:49, 9 November 2021
Sebaceous carcinoma, also known as sebaceous cell carcinoma, is an uncommon skin tumour.
| Sebaceous carcinoma | |
|---|---|
| Diagnosis in short | |
|
Template:Px Sebaceous carcinoma. H&E stain. | |
|
| |
| LM |
sebaceous differentiation (may be a minor component): sebocytes (abundant pale fluffy cytoplasm with vacuolization); basaloid cells (often dominant); nodular or diffuse growth pattern surrounded by a dense fibrous stroma; infiltrative border; +/-nuclear atypia, +/-squamous differentiation, +/-foreign body-type giant cells |
| LM DDx | sebaceous adenoma, squamous cell carcinoma (clear cell variant), malignant melanoma, extramammary Paget disease, trichoblastoma,basal cell carcinoma, sweat gland carcinoma |
| IHC | EMA +ve (only sebaceous component), CEA -ve |
| Gross | yellow or red (ulcerated) nodule |
| Site | skin - usu. head and neck, salivary gland |
|
| |
| Syndromes | Muir-Torre syndrome |
|
| |
| Prevalence | uncommon |
General
- Malignant.
- May arise in a salivary gland.[1]
- Can be part of Muir-Torre syndrome.
Notes:
- Sebaceous lesions (from benign to malignant): sebaceous hyperplasia, sebaceous adenoma, sebaceoma, sebaceous carcinoma.
Gross
Features:[2]
- Classically head and neck tumour.
- Yellow or red (ulcerated) nodule.
Microscopic
Features:[3]
- Sebaceous differentiation - may be a minor component - key feature.
- Sebocytes = abundant pale fluffy cytoplasm with vacuolization.
- Basaloid cells - often dominant.
- May lead to confusion with basaloid tumours.
- Nodular or diffuse growth pattern surrounded by a dense fibrous stroma.
- Infiltrative border - important.
- The key difference with sebaceous adenoma in cases where there isn't significant nuclear atypia.
- +/-Nuclear atypia.
- +/-Squamous differentiation.
- +/-Foreign body-type giant cells.
DDx:
- Sebaceous adenoma - non-infiltrative border.
- Squamous cell carcinoma, clear cell variant.
- Malignant melanoma.
- Extramammary Paget disease.
- Trichoblastoma.
- Basal cell carcinoma.
- Sweat gland carcinoma.
Images

Sebaceous carcinoma - intermed. mag. (WC/Nephron)
- Sebaceous carcinoma - high mag.jpg
Sebaceous carcinoma - high mag. (WC/Nephron)
Sebaceous carcinoma - very high mag. (WC/Nephron)


{kind=link}
www:
{kind=link}
Grading
Three tier system:[3]
- Well-differentiated - sebocytes predominant.
- Moderately differentiated - sebocytes are easily recognized but a minor component.
- Poorly differentiated - sebocytes are rare.
IHC
Features:[3]
- CK7 +ve[4] - often weak.
- EMA +ve -- only sebaceous component.[5]
- CEA -ve.
- Positive in extramammary Paget disease, sweat duct tumours.
Images:
{kind=link}
Sebaceous carcinoma versus squamous cell carcinoma
- CK7 +ve.
- Useful if positive: 24 of 27 sebaceous carcinomas +ve; only 2 of 22 squamous cell carcinomas +ve.[6]
- Ber-EP4 -ve/+ve.
- Useful if positive: 7 of 27 sebaceous carcinomas +ve; 0 of 22 squamous cell carcinomas +ve.[6]
- EMA +ve.
- Useful if negative: 27 of 27 sebaceous carcinoma +ve; 16 of 22 squamous cell carcinoma +ve.[6]
Sign out
SKIN LESION, NOSE, BIOPSY: - SEBACEOUS CARCINOMA, WELL-DIFFERENTIATED, COMPLETELY EXCISED IN THE PLANE OF SECTION. COMMENT: EMA staining marks the sebocytes. The lesion is negative for Ber-EP4. Sebaceous carcinoma may be seen in the context of Muir-Torre syndrome.
Micro
Well differentiated
The sections show well-circumscribed dermal nests of basaloid cells with peripheral palisading, surrounded by a dense fibrous stroma. The basaloid cells have distinct nucleoli. Focally, the basaloid nests contain small clusters of cells with abundant pale, vacuolated, fluffy-appearing cytoplasm (sebocytes). Mitotic activity is minimal.
There is no artefactual clefting between the stroma and basaloid cell nests. The epidermis matures to the surface and does not have basal atypia.
The lesion is completely excised in the plane of section.
Poor differentiated
The sections show well-circumscribed dermal nests of basaloid cells with peripheral palisading, surrounded by a dense fibrous stroma, that extend from the skin surface almost to the adipose tissue. The basaloid cells have moderate nuclear atypia with occasional monstrous cells. Mitotic activity is abundant and atypical mitoses are present. The nests contain rare cells with pale, fluffy-appearing cytoplasm, suggestive of sebocytes.
See also
References
- ↑ 1.0 1.1 URL: http://www.ispub.com/journal/the_internet_journal_of_otorhinolaryngology/volume_9_number_2_11/article/sebaceous_adenocarcinoma_of_the_parotid_gland_a_case_report_and_literature_review.html. Accessed on: 8 September 2011.
- ↑ Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 431. ISBN 978-0443066542.
- ↑ 3.0 3.1 3.2 Busam, Klaus J. (2009). Dermatopathology: A Volume in the Foundations in Diagnostic Pathology Series (1st ed.). Saunders. pp. 431-2. ISBN 978-0443066542.
- ↑ Ansai, S.; Arase, S.; Kawana, S.; Kimura, T. (Oct 2011). "Immunohistochemical findings of sebaceous carcinoma and sebaceoma: retrieval of cytokeratin expression by a panel of anti-cytokeratin monoclonal antibodies.". J Dermatol 38 (10): 951-8. doi:10.1111/j.1346-8138.2011.01274.x. PMID 21592202.
- ↑ 5.0 5.1 Sinard, JH. (Jun 1999). "Immunohistochemical distinction of ocular sebaceous carcinoma from basal cell and squamous cell carcinoma.". Arch Ophthalmol 117 (6): 776-83. PMID 10369589.
- ↑ 6.0 6.1 6.2 Plaza JA, Mackinnon A, Carrillo L, Prieto VG, Sangueza M, Suster S (November 2015). "Role of immunohistochemistry in the diagnosis of sebaceous carcinoma: a clinicopathologic and immunohistochemical study". Am J Dermatopathol 37 (11): 809–21. doi:10.1097/DAD.0000000000000255. PMID 26485238.