Difference between revisions of "Abdominoperineal resection grossing"
Jump to navigation
Jump to search
(remove broken image link) |
|||
| (7 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
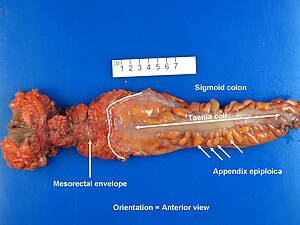
[[Image:Rectum - anterior view.jpg|right|thumb|An addominoperineal resection specimen prior to opening and [[inking]].]] | |||
This protocol deals with '''abdominoperineal resection grossing'''. | This protocol deals with '''abdominoperineal resection grossing'''. | ||
| Line 4: | Line 5: | ||
==Introduction== | ==Introduction== | ||
This is a relatively uncommon specimen. APRs are done for distal [[colorectal carcinoma|rectal cancer]]s when a [[lower anterior resection]] is not feasible. | This is a relatively uncommon specimen. APRs are done for distal [[colorectal carcinoma|rectal cancer]]s when a [[lower anterior resection]] (LAR) is not feasible. | ||
LAR are the preferred surgery for rectal cancer, as individuals post-APR are left with a permanent [[stoma]] and expel fecal material into a bag. | |||
==Protocol== | ==Protocol== | ||
| Line 15: | Line 18: | ||
*Circumference - distal end: ___ cm. | *Circumference - distal end: ___ cm. | ||
*Rectum length (distal margin to mesorectal reflection): ___ cm. | *Rectum length (distal margin to mesorectal reflection): ___ cm. | ||
*Skin (anal): ___ cm. | |||
Appearance - external: | Appearance - external: | ||
| Line 53: | Line 57: | ||
===Alternate approaches=== | ===Alternate approaches=== | ||
==See also== | ==See also== | ||
*[[Sigmoidectomy for diverticular disease]]. | |||
*[[Donuts]]. | |||
*[[Rectum]]. | |||
===Related protocols=== | ===Related protocols=== | ||
*[[Lower anterior resection for cancer grossing]]. | *[[Lower anterior resection for cancer grossing]]. | ||
| Line 60: | Line 69: | ||
{{Reflist|1}} | {{Reflist|1}} | ||
[[Category:Gastrointestinal pathology]] | [[Category:Gastrointestinal pathology]] | ||
[[Category:Gross pathology]] | [[Category:Gross pathology]] | ||
Latest revision as of 14:11, 15 October 2024

An addominoperineal resection specimen prior to opening and inking.
This protocol deals with abdominoperineal resection grossing.
Abdominoperineal resection, abbreviated APR, is also written as abdominal perineal resection.
Introduction
This is a relatively uncommon specimen. APRs are done for distal rectal cancers when a lower anterior resection (LAR) is not feasible.
LAR are the preferred surgery for rectal cancer, as individuals post-APR are left with a permanent stoma and expel fecal material into a bag.
Protocol
Specimen:
- Abdominoperineal resection.
Dimensions:
- Length: ___ cm.
- Circumference - proximal end: ___ cm.
- Circumference - distal end: ___ cm.
- Rectum length (distal margin to mesorectal reflection): ___ cm.
- Skin (anal): ___ cm.
Appearance - external:
- Completeness of mesorectal excision: [complete].
- Serosal aspect of bowel: [shiny].
- Perforation: [present/not present].
Inking:
- Circumferential margin: [black].
- Serosal puckering: [blue].
Tumour characteristics:
- Dimensions (along axis, circumferential, depth): ___ x ___ x ___ cm.
- Distance to nearest mucosal margin: ___ cm, [distal] margin.
- Distance to circumferential margin: ___ cm.
- Circumferential location: [anterior/left/right/posterior/circumferential].
Representative sections are submitted as follows:
- Proximal margin. ‡
- Distal margin. ‡
- Tumour - deepest invasion.
- Additional sections of tumour (1 section/cm).
- All polyps (if less than 10).
- Normal appearing mucosa.
- Lymph nodes. †
Protocol notes
- ‡ Usually submitted completely and en face; if the margin is close (<2 cm) on edge is typically preferred.
- † Recommended minimum number of lymph nodes is 12.[1]
Images

APR specimen - anterior view. (WC/Hagemani)

APR specimen - lateral. (WC/Hagemani)

APR specimen - inked (WC/Hagemani)

APR specimen - opened (WC/Hagemani)



Alternate approaches
See also
Related protocols
References
- ↑ Ihnát, P.; Delongová, P.; Horáček, J.; Ihnát Rudinská, L.; Vávra, P.; Zonča, P. (Sep 2014). "The Impact of Standard Protocol Implementation on the Quality of Colorectal Cancer Pathology Reporting.". World J Surg. doi:10.1007/s00268-014-2796-4. PMID 25234197.