Difference between revisions of "Wilson's disease"
(→Microscopic: added a case) |
|||
| (5 intermediate revisions by 2 users not shown) | |||
| Line 22: | Line 22: | ||
*[[Steatosis of the liver|Steatosis]]. | *[[Steatosis of the liver|Steatosis]]. | ||
*Portal fibrosis. | *Portal fibrosis. | ||
A. [[File:1 Wilson 1 680x512px.tif|Inflamed & relatively unaffected segments (40X).]]<br> | |||
B. [[File:2 Wilson 1 680x512px.tif|Bile ductular proliferation with interface hepatitis [inflammation of periportal hepatocytes] (200X).]]<br> | |||
C. [[File:3 Wilson 1 680x512px.tif|Enlarged hepatocytes, some with feathery degeneration, others with steatosis. Nuclei show nucleoli (400X).]]<br> | |||
D. [[File:4 Wilson 1 680x512px.tif|Trichrome shows periportal & sinusoidal fibrosis. No bridging was seen. (100X).]]<br> | |||
Wilson’s disease, pre-cirrhotic. A. Inflamed & relatively unaffected segments. B. Bile ductular proliferation with interface hepatitis [inflammation of periportal hepatocytes]. C. Enlarged hepatocytes, some with feathery degeneration, others with steatosis. Nuclei show nucleoli. D. Trichrome shows periportal & sinusoidal fibrosis. | |||
[[File:4 38555059990939 sl 1.png|Wilson’s disease with cirrhosis]] | |||
[[File:4 38555059990939 sl 2.png|Wilson’s disease with cirrhosis]] | |||
[[File:4 38555059990939 sl 3.png|Wilson’s disease with cirrhosis]] | |||
[[File:4 38555059990939 sl 4.png|Wilson’s disease with cirrhosis]] | |||
[[File:4 38555059990939 sl 5.png|Wilson’s disease with cirrhosis]] <br> | |||
Wilson’s disease with cirrhosis in a 22 year old woman. A. Nodules show steatosis without definite triads. B. Trichrome shows minute fibrous bound nodules in this case. C. Reticulin shows extensive regeneration (2-3 nuclei thick cords with lack of direction) with nodule formation. D. Bridge with extensive proliferated bile ductules and acute and chronic inflammatory cells. E. Ballooning degeneration with Mallory bodies. | |||
==Stains== | ==Stains== | ||
| Line 38: | Line 51: | ||
*Atomic absorption spectroscopy. | *Atomic absorption spectroscopy. | ||
**>250 microg of copper/g of liver suggest Wilson's disease; below does not exclude it.<ref name=pmid16234011>{{Cite journal | last1 = Ferenci | first1 = P. | last2 = Steindl-Munda | first2 = P. | last3 = Vogel | first3 = W. | last4 = Jessner | first4 = W. | last5 = Gschwantler | first5 = M. | last6 = Stauber | first6 = R. | last7 = Datz | first7 = C. | last8 = Hackl | first8 = F. | last9 = Wrba | first9 = F. | title = Diagnostic value of quantitative hepatic copper determination in patients with Wilson's Disease. | journal = Clin Gastroenterol Hepatol | volume = 3 | issue = 8 | pages = 811-8 | month = Aug | year = 2005 | doi = | PMID = 16234011 }}</ref> | **>250 microg of copper/g of liver suggest Wilson's disease; below does not exclude it.<ref name=pmid16234011>{{Cite journal | last1 = Ferenci | first1 = P. | last2 = Steindl-Munda | first2 = P. | last3 = Vogel | first3 = W. | last4 = Jessner | first4 = W. | last5 = Gschwantler | first5 = M. | last6 = Stauber | first6 = R. | last7 = Datz | first7 = C. | last8 = Hackl | first8 = F. | last9 = Wrba | first9 = F. | title = Diagnostic value of quantitative hepatic copper determination in patients with Wilson's Disease. | journal = Clin Gastroenterol Hepatol | volume = 3 | issue = 8 | pages = 811-8 | month = Aug | year = 2005 | doi = | PMID = 16234011 }}</ref> | ||
[[Sensitivity]]:<ref>{{Cite journal | last1 = Liggi | first1 = M. | last2 = Mais | first2 = C. | last3 = Demurtas | first3 = M. | last4 = Sorbello | first4 = O. | last5 = Demelia | first5 = E. | last6 = Civolani | first6 = A. | last7 = Demelia | first7 = L. | title = Uneven distribution of hepatic copper concentration and diagnostic value of double-sample biopsy in Wilson's disease. | journal = Scand J Gastroenterol | volume = 48 | issue = 12 | pages = 1452-8 | month = Dec | year = 2013 | doi = 10.3109/00365521.2013.845904 | PMID = 24164422 }}</ref> | |||
*250 microg of copper/g of liver - 80-86% (value dependent on sampling). | |||
*50 microg of copper/g of liver - 97%. | |||
==See also== | ==See also== | ||
Latest revision as of 19:17, 9 January 2017
Wilson disease's is a rare autosomal recessive genetic disease characterized by abnormal copper transportation. Its' presentation may be atypical. In the context of pathology, it is typically seen as a liver biopsy.
General
Epidemiology:
- Rare autosomal recessive - mutation in copper-transporting adenosine triphosphatase (ATPase) gene (ATP7B).[1][2]
- Heterozygote carrier rate approximately 1/100 persons.[1]
- Young individuals - usually 12-23 years old.
- May have late-onset (symptomatic when >40 years old).[3]
Clinical:
- Kayser-Fleischer rings --> on slit-lamp examination (green eyes).
- May present to psychiatry or appear to be abusing EtOH.
- Serum ceruloplasmin - lower than normal; typical value for Wilson's ~ 0.12 g/L.
- <0.20 g/L is a criteria for Wilson's disease.[4]
Etiology:
- Excess copper -- due to genetic defect.
Microscopic
Features:
- Nothing specific - known as the great mimicker of liver pathology.
- Steatosis.
- Portal fibrosis.
A. 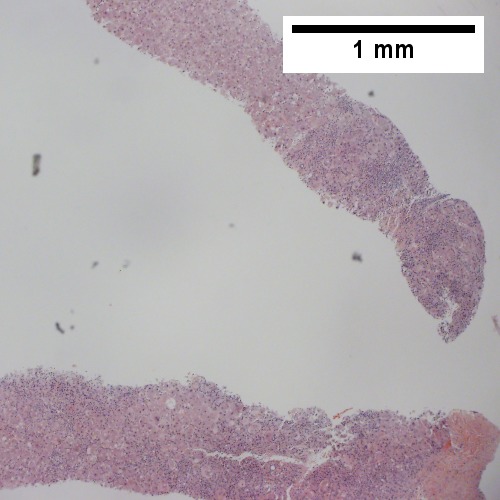
B. ![Bile ductular proliferation with interface hepatitis [inflammation of periportal hepatocytes] (200X).](/w/images/thumb/4/41/2_Wilson_1_680x512px.tif/lossy-page1-500px-2_Wilson_1_680x512px.tif.jpg)
C. 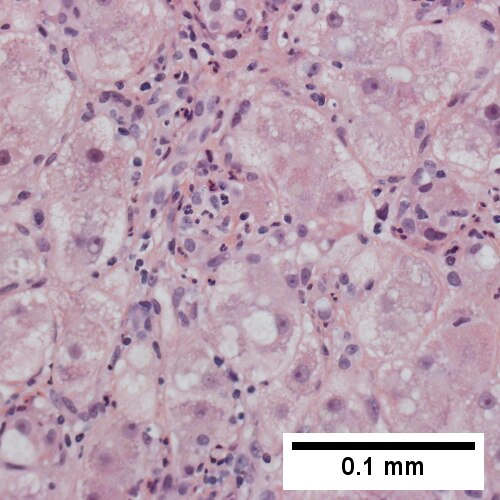
D. 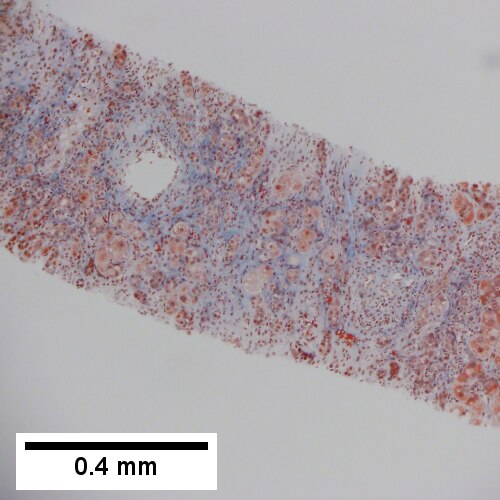
Wilson’s disease, pre-cirrhotic. A. Inflamed & relatively unaffected segments. B. Bile ductular proliferation with interface hepatitis [inflammation of periportal hepatocytes]. C. Enlarged hepatocytes, some with feathery degeneration, others with steatosis. Nuclei show nucleoli. D. Trichrome shows periportal & sinusoidal fibrosis.





Wilson’s disease with cirrhosis in a 22 year old woman. A. Nodules show steatosis without definite triads. B. Trichrome shows minute fibrous bound nodules in this case. C. Reticulin shows extensive regeneration (2-3 nuclei thick cords with lack of direction) with nodule formation. D. Bridge with extensive proliferated bile ductules and acute and chronic inflammatory cells. E. Ballooning degeneration with Mallory bodies.
Stains
- Copper staining positive - only 15% of cases.
- Other stains: rhodinine (red/orange granules = positive), orecin.
Notes:
- Copper staining is a non-specific finding seen in many liver diseases; it is associated with impaired bile secretion.[5]
Image
Additional testing
Copper quantification:
- Mass spectrometry.[6]
- Atomic absorption spectroscopy.
- >250 microg of copper/g of liver suggest Wilson's disease; below does not exclude it.[7]
- 250 microg of copper/g of liver - 80-86% (value dependent on sampling).
- 50 microg of copper/g of liver - 97%.
See also
References
- ↑ 1.0 1.1 http://emedicine.medscape.com/article/183456-overview
- ↑ Online 'Mendelian Inheritance in Man' (OMIM) 606882
- ↑ Ferenci, P.; Członkowska, A.; Merle, U.; Ferenc, S.; Gromadzka, G.; Yurdaydin, C.; Vogel, W.; Bruha, R. et al. (Apr 2007). "Late-onset Wilson's disease.". Gastroenterology 132 (4): 1294-8. doi:10.1053/j.gastro.2007.02.057. PMID 17433323.
- ↑ Diagnostic accuracy of serum ceruloplasmin in Wilson disease: determination of sensitivity and specificity by ROC curve analysis among ATP7B-genotyped subjects. Mak CM, Lam CW, Tam S. Clin Chem. 2008 Aug;54(8):1356-62. Epub 2008 Jun 12. PMID 18556333. URL: http://www.clinchem.org/cgi/reprint/54/8/1356.pdf. Accessed on: 28 September 2009.
- ↑ Miyamura H, Nakanuma Y, Kono N (December 1988). "Survey of copper granules in liver biopsy specimens from various liver abnormalities other than Wilson's disease and biliary diseases". Gastroenterol. Jpn. 23 (6): 633–8. PMID 2464523.
- ↑ Hahn, SH. (May 2014). "Population screening for Wilson's disease.". Ann N Y Acad Sci 1315: 64-9. doi:10.1111/nyas.12423. PMID 24731025.
- ↑ Ferenci, P.; Steindl-Munda, P.; Vogel, W.; Jessner, W.; Gschwantler, M.; Stauber, R.; Datz, C.; Hackl, F. et al. (Aug 2005). "Diagnostic value of quantitative hepatic copper determination in patients with Wilson's Disease.". Clin Gastroenterol Hepatol 3 (8): 811-8. PMID 16234011.
- ↑ Liggi, M.; Mais, C.; Demurtas, M.; Sorbello, O.; Demelia, E.; Civolani, A.; Demelia, L. (Dec 2013). "Uneven distribution of hepatic copper concentration and diagnostic value of double-sample biopsy in Wilson's disease.". Scand J Gastroenterol 48 (12): 1452-8. doi:10.3109/00365521.2013.845904. PMID 24164422.