Difference between revisions of "Uterine prolapse"
Jump to navigation
Jump to search
(redirect) |
|||
| (6 intermediate revisions by the same user not shown) | |||
| Line 1: | Line 1: | ||
'''Uterine prolapse''' is a frequent benign pathology of the [[uterus]] and a common reason for [[hysterectomy]]. | |||
==General== | |||
*[[Clinical diagnosis]]. | |||
*A common indication for a total hysterectomy. | |||
*Hysterectomy specimen usually comes with some [[vagina]]l mucosa. | |||
*Parous women, usually menopausal.<ref name=pmid20607975>{{Cite journal | last1 = Mladenović-Segedi | first1 = L. | last2 = Segedi | first2 = D. | title = [Most important etiologic factors in the development of genital prolapse]. | journal = Srp Arh Celok Lek | volume = 138 | issue = 5-6 | pages = 315-8 | month = | year = | doi = | PMID = 20607975 }}</ref> | |||
*Possibly [[obesity]] - studies vary.<ref name=pmid22732579 >{{Cite journal | last1 = Thubert | first1 = T. | last2 = Deffieux | first2 = X. | last3 = Letouzey | first3 = V. | last4 = Hermieu | first4 = JF. | title = [Obesity and urogynecology: a systematic review]. | journal = Prog Urol | volume = 22 | issue = 8 | pages = 445-53 | month = Jul | year = 2012 | doi = 10.1016/j.purol.2012.03.009 | PMID = 22732579 }}</ref> | |||
==Gross== | |||
*Long cervix. | |||
==Microscopic== | |||
Features: | |||
*Uterus: non-specific. | |||
*Vaginal mucosa: (focal) keratinization due to rubbing - '''common finding'''. | |||
Note: | |||
*Benign stromal atypia may be seen.<ref name=pmid10680891>{{Cite journal | last1 = Nucci | first1 = MR. | last2 = Young | first2 = RH. | last3 = Fletcher | first3 = CD. | title = Cellular pseudosarcomatous fibroepithelial stromal polyps of the lower female genital tract: an underrecognized lesion often misdiagnosed as sarcoma. | journal = Am J Surg Pathol | volume = 24 | issue = 2 | pages = 231-40 | month = Feb | year = 2000 | doi = | PMID = 10680891 }}</ref><ref>{{Cite journal | last1 = Rodrigues | first1 = MI ''et al.'' | last2 = | first2 = | title = Atypical stromal cells as a diagnostic pitfall in lesions of the lower | |||
female genital tract and uterus: a review and presentation of some unusual cases | journal = Patología | volume = 47 | issue = 2 | pages = 103-7 | month = April-June | year = 2009 | doi = | PMID = | PMC = | url = http://www.medigraphic.com/pdfs/patrevlat/rlp-2009/rlp092e.pdf }}</ref> | |||
===Images=== | |||
<gallery> | |||
Image: Keratinized cervix -- intermed mag.jpg | Keratinized cervix - intermed. mag. (WC) | |||
Image: Keratinized cervix -- high mag.jpg | Keratinized cervix - high mag. (WC) | |||
Image: Keratinized cervix -- very high mag.jpg | Keratinized cervix - very high mag. (WC) | |||
</gallery> | |||
==Sign out== | |||
<pre> | |||
Uterus, Cervix and Vagina Mucosa, Total Hysterectomy: | |||
- Uterine cervix with focal keratinization, otherwise within normal limits. | |||
- Inactive endometrium. | |||
- Squamous mucosa with keratinization, consistent with prolapse-associated | |||
changes in the vagina. | |||
- Medial calcific sclerosis. | |||
- Atherosclerosis, moderate-to-severe. | |||
- NEGATIVE for malignancy. | |||
</pre> | |||
<pre> | |||
Submitted as "Uterine Cervix", Excision: | |||
- Squamous mucosa with hyperplasia, parakeratosis, and stromal atypia, see comment. | |||
- NEGATIVE for dysplasia and NEGATIVE for evidence of malignancy. | |||
Comment: | |||
The stromal atypia is favoured to be benign change, as it is without significant proliferation, | |||
not mass forming and near the stromal-epithelial interface. | |||
The stromal cells stain as follows: | |||
POSITIVE: vimentin, ER. | |||
NEGATIVE: AE1/AE3, CD10. | |||
PROLIFERATION (Ki-67): <1%. | |||
</pre> | |||
===Block letters=== | |||
<pre> | |||
UTERUS AND CERVIX, TOTAL HYSTERECTOMY: | |||
- UTERINE CERVIX WITH FOCAL KERATINIZATION OTHERWISE WITHIN NORMAL LIMITS. | |||
- NONPROLIFERATIVE ENDOMETRIUM. | |||
</pre> | |||
<pre> | |||
UTERUS AND CERVIX, TOTAL HYSTERECTOMY: | |||
- UTERINE CERVIX WITH KERATINIZATION, OTHERWISE WITHIN NORMAL LIMITS. | |||
- CYSTIC NONPROLIFERATIVE ENDOMETRIUM. | |||
- UTERINE SMOOTH MUSCLE AND SEROSA WITHIN NORMAL LIMITS. | |||
- NEGATIVE FOR MALIGNANCY. | |||
</pre> | |||
===Denudated exocervix=== | |||
<pre> | |||
UTERUS AND CERVIX, TOTAL HYSTERECTOMY: | |||
- UTERINE CERVIX WITH MILD CHRONIC INFLAMMATION AND EXOCERVICAL DENUDATION, | |||
NO EVIDENCE OF DYSPLASIA. | |||
- CYSTIC NONPROLIFERATIVE ENDOMETRIUM. | |||
- UTERINE CORPUS WITH BENIGN HYALINIZED NODULE. | |||
- NEGATIVE FOR MALIGNANCY. | |||
COMMENT: | |||
Levels were cut on the uterine cervix sections (A1 and A2). | |||
</pre> | |||
===Focal ulceration=== | |||
<pre> | |||
- UTERINE CERVIX WITH PARAKERATOSIS, ACANTHOSIS, CHRONIC INFLAMMATION, AND FOCAL | |||
ULCERATION ASSOCIATED WITH GRANULATION TISSUE FORMATION. | |||
- PARTIALLY CYSTIC NONPROLIFERATIVE ENDOMETRIUM. | |||
- UTERINE CORPUS WITH LEIOMYOMA. | |||
- NO EVIDENCE OF DYSPLASIA. | |||
- NEGATIVE FOR HYPERPLASIA AND NEGATIVE FOR MALIGNANCY. | |||
</pre> | |||
===With endometrial polyp=== | |||
<pre> | |||
UTERUS AND CERVIX, TOTAL HYSTERECTOMY: | |||
- BENIGN ENDOMETRIAL POLYP WITH NONPROLIFERATIVE ENDOMETRIAL GLANDS. | |||
- UTERINE CERVIX WITH MILD CHRONIC INFLAMMATION AND FOCAL EXOCERVICAL DENUDATION, | |||
NO EVIDENCE OF DYSPLASIA. | |||
- VERY WEAKLY PROLIFERATIVE ENDOMETRIUM, MOSTLY ATROPHIC APPEARING, NEGATIVE FOR | |||
ENDOMETRIAL HYPERPLASIA. | |||
- UTERINE CORPUS WITHIN NORMAL LIMITS. | |||
- NEGATIVE FOR MALIGNANCY. | |||
</pre> | |||
==See also== | |||
*[[Uterus]]. | |||
*[[Prolapse]]. | |||
==References== | |||
{{Reflist|2}} | |||
[[Category:Diagnosis]] | [[Category:Diagnosis]] | ||
[[Category:Gynecologic pathology]] | |||
Latest revision as of 19:10, 8 July 2016
Uterine prolapse is a frequent benign pathology of the uterus and a common reason for hysterectomy.
General
- Clinical diagnosis.
- A common indication for a total hysterectomy.
- Hysterectomy specimen usually comes with some vaginal mucosa.
- Parous women, usually menopausal.[1]
- Possibly obesity - studies vary.[2]
Gross
- Long cervix.
Microscopic
Features:
- Uterus: non-specific.
- Vaginal mucosa: (focal) keratinization due to rubbing - common finding.
Note:
Images
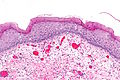
Keratinized cervix - intermed. mag. (WC)

Keratinized cervix - high mag. (WC)

Keratinized cervix - very high mag. (WC)



Sign out
Uterus, Cervix and Vagina Mucosa, Total Hysterectomy: - Uterine cervix with focal keratinization, otherwise within normal limits. - Inactive endometrium. - Squamous mucosa with keratinization, consistent with prolapse-associated changes in the vagina. - Medial calcific sclerosis. - Atherosclerosis, moderate-to-severe. - NEGATIVE for malignancy.
Submitted as "Uterine Cervix", Excision: - Squamous mucosa with hyperplasia, parakeratosis, and stromal atypia, see comment. - NEGATIVE for dysplasia and NEGATIVE for evidence of malignancy. Comment: The stromal atypia is favoured to be benign change, as it is without significant proliferation, not mass forming and near the stromal-epithelial interface. The stromal cells stain as follows: POSITIVE: vimentin, ER. NEGATIVE: AE1/AE3, CD10. PROLIFERATION (Ki-67): <1%.
Block letters
UTERUS AND CERVIX, TOTAL HYSTERECTOMY: - UTERINE CERVIX WITH FOCAL KERATINIZATION OTHERWISE WITHIN NORMAL LIMITS. - NONPROLIFERATIVE ENDOMETRIUM.
UTERUS AND CERVIX, TOTAL HYSTERECTOMY: - UTERINE CERVIX WITH KERATINIZATION, OTHERWISE WITHIN NORMAL LIMITS. - CYSTIC NONPROLIFERATIVE ENDOMETRIUM. - UTERINE SMOOTH MUSCLE AND SEROSA WITHIN NORMAL LIMITS. - NEGATIVE FOR MALIGNANCY.
Denudated exocervix
UTERUS AND CERVIX, TOTAL HYSTERECTOMY: - UTERINE CERVIX WITH MILD CHRONIC INFLAMMATION AND EXOCERVICAL DENUDATION, NO EVIDENCE OF DYSPLASIA. - CYSTIC NONPROLIFERATIVE ENDOMETRIUM. - UTERINE CORPUS WITH BENIGN HYALINIZED NODULE. - NEGATIVE FOR MALIGNANCY. COMMENT: Levels were cut on the uterine cervix sections (A1 and A2).
Focal ulceration
- UTERINE CERVIX WITH PARAKERATOSIS, ACANTHOSIS, CHRONIC INFLAMMATION, AND FOCAL ULCERATION ASSOCIATED WITH GRANULATION TISSUE FORMATION. - PARTIALLY CYSTIC NONPROLIFERATIVE ENDOMETRIUM. - UTERINE CORPUS WITH LEIOMYOMA. - NO EVIDENCE OF DYSPLASIA. - NEGATIVE FOR HYPERPLASIA AND NEGATIVE FOR MALIGNANCY.
With endometrial polyp
UTERUS AND CERVIX, TOTAL HYSTERECTOMY: - BENIGN ENDOMETRIAL POLYP WITH NONPROLIFERATIVE ENDOMETRIAL GLANDS. - UTERINE CERVIX WITH MILD CHRONIC INFLAMMATION AND FOCAL EXOCERVICAL DENUDATION, NO EVIDENCE OF DYSPLASIA. - VERY WEAKLY PROLIFERATIVE ENDOMETRIUM, MOSTLY ATROPHIC APPEARING, NEGATIVE FOR ENDOMETRIAL HYPERPLASIA. - UTERINE CORPUS WITHIN NORMAL LIMITS. - NEGATIVE FOR MALIGNANCY.
See also
References
- ↑ Mladenović-Segedi, L.; Segedi, D.. "[Most important etiologic factors in the development of genital prolapse].". Srp Arh Celok Lek 138 (5-6): 315-8. PMID 20607975.
- ↑ Thubert, T.; Deffieux, X.; Letouzey, V.; Hermieu, JF. (Jul 2012). "[Obesity and urogynecology: a systematic review].". Prog Urol 22 (8): 445-53. doi:10.1016/j.purol.2012.03.009. PMID 22732579.
- ↑ Nucci, MR.; Young, RH.; Fletcher, CD. (Feb 2000). "Cellular pseudosarcomatous fibroepithelial stromal polyps of the lower female genital tract: an underrecognized lesion often misdiagnosed as sarcoma.". Am J Surg Pathol 24 (2): 231-40. PMID 10680891.
- ↑ Rodrigues, MI et al. (April-June 2009). [http://www.medigraphic.com/pdfs/patrevlat/rlp-2009/rlp092e.pdf "Atypical stromal cells as a diagnostic pitfall in lesions of the lower female genital tract and uterus: a review and presentation of some unusual cases"]. Patología 47 (2): 103-7. http://www.medigraphic.com/pdfs/patrevlat/rlp-2009/rlp092e.pdf.