Wilms tumour
Jump to navigation
Jump to search
The printable version is no longer supported and may have rendering errors. Please update your browser bookmarks and please use the default browser print function instead.
| Wilms tumour | |
|---|---|
| Diagnosis in short | |
 Wilms tumour. H&E stain. | |
|
| |
| Synonyms | nephroblastoma |
| LM DDx | metanephric adenoma, nephrogenic nests, small round cell tumours, Immature teratoma |
| IHC | WT-1 +ve, CD56 +ve |
| Site | kidney - see pediatric kidney tumours |
|
| |
| Syndromes | WAGR syndrome, Beckwith-Wiedemann syndrome, Denys-Drash syndrome |
|
| |
| Signs | +/-abdominal mass |
| Prevalence | most common pediatric kidney tumour |
Wilms tumour, also nephroblastoma and Wilms' tumour, is the most common pediatric kidney tumour.[1][2]
General
- Common abdominal pediatric tumour.
- Affects approximately 1 in 8000 children.
- There is no sex predilection and the mean patient age at diagnosis ranges among 37 to 43 months.
- May be associated with a syndrome:[3]
- WAGR syndrome (Wilms tumour, Aniridia (absence of iris), GU abnormalities, Retardation).[4]
- Beckwith-Wiedemann syndrome.[5]
- Denys-Drash syndrome.[6]
Gross
Features [7]
- Most nephroblastomas are unifocal.
- Usually solitary, rounded, multilobular masses sharply demarcated from adjacent parenchyma.
- The cut surface is most commonly pale grey or tan.
- Cyst most be prominent in some cases.
- Multifocal masses in a single kidney and bilateral primary lesions are less frequent.
Images
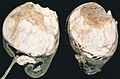
Wilms tumour. (WC/AFIP)

www:
Microscopic
Features - classically three components (blastema, immature stroma, tubules):[8]
- Malignant small round blue cells ("blastema"):
- The blastemal component is the least differentiated cellular element.
- Size = ~ 2x RBC diameter.
- Nuclear pleomorphism (variation of size, shape and staining).
- Irregular nuclear membrane - important.
- Scant/difficult to discern cytoplasm - basophilic (light blue).
- Mitoses - common.
- Stroma ("immature stroma"):
- Spindle cells:
- Elliptical nuclear membrane.
- Abundant loose cytoplasm.
- Spindle cells:
- Epithelial components ("tubules"):
- Primitive rossete-like tubules, well-formed maturing and mature tubules, glomerular structures and variably papillary architecture.
- Usually clustered.
- Usu. have a central (clear/white) space surrounded by a rim of intensely eosinophilic cytoplasm.
- Nuclei of tubular structures often elongated and palisaded.
- Primitive rossete-like tubules, well-formed maturing and mature tubules, glomerular structures and variably papillary architecture.
Other findings:
- Commonly seen in association with nephrogenic rests.
- Cluster of cells small (blue) cells; lack nuclear atypia seen in Wilms tumour.[9]
- +/-Heterologous elements (skeletal muscle, smooth muscle adipose tissue, cartilage).[10]
- Heterologous = doesn't normally belong there.[11]
DDx:
- Metanephric adenoma.
- Nephrogenic nests.
- Other small round cell tumours.
- Synovial sarcoma, biphasic - especially in adults.
- Immature teratoma.
Notes:
- Palisade = fence made of stakes driven into the ground.[12]
- Approximately 30-40% Wilms tumour cases have nephrogenic rests.[13]
- The three phases are also called blastemal, epithelial and stromal.[10]
Images
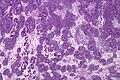
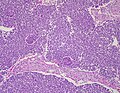
Wilms tumour - low mag. (WC/Nephron)
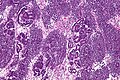
Wilms tumour - intermed. mag. (WC/Nephron)
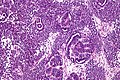
Wilms tumour - high mag. (WC/Nephron)
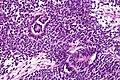
Wilms tumour - very high mag. (WC/Nephron)
Wilms tumor - low mag. (WC/Ed Uthman)



_(4882456062).jpg)
www:
{kind=link}
Anaplasia
Subclassified as:[10]
- Focal anaplasia.
- Diffuse anaplasia.
Criteria (all of the following):[10]
- Atypical mitoses.
- Nuclear hyperchromasia.
- Nuclear size variation (of the tumour cells) > 3x.
IHC
- WT-1 +ve (nuclear).
- CD56 +ve.[14]
- -ve in metanephric adenoma.
Molecular
- Cytogenetics[15]
- Partial gains of 1q.
- Partial losses of 1p, 1q, 4q, 11q, 16q, 22q.
- Complete loss of chromosome 16, 11, 12, 22.
- Trisomy of chromosome 8, 12, 13, 18.
See also
References
- ↑ Coppes MJ, Wolff JE, Ritchey ML (1999). "Wilms tumour: diagnosis and treatment". Paediatr Drugs 1 (4): 251–62. PMID 10935424.
- ↑ Stefanowicz J, Sierota D, Balcerska A, Stoba C (2004). "[Wilms' tumour of unfavorable histology--results of treatment with the SIOP 93-01 protocol at the Gdańsk centre. Preliminary report]" (in Polish). Med Wieku Rozwoj 8 (2 Pt 1): 197–200. PMID 15738594.
- ↑ URL: http://emedicine.medscape.com/article/989398-overview. Accessed on: 9 March 2011.
- ↑ Online 'Mendelian Inheritance in Man' (OMIM) 194072
- ↑ Online 'Mendelian Inheritance in Man' (OMIM) 130650
- ↑ Online 'Mendelian Inheritance in Man' (OMIM) 194080
- ↑ Coppes, MJ.; Arnold, M.; Beckwith, JB.; Ritchey, ML.; D'Angio, GJ.; Green, DM.; Breslow, NE. (Apr 1999). "Factors affecting the risk of contralateral Wilms tumor development: a report from the National Wilms Tumor Study Group.". Cancer 85 (7): 1616-25. PMID 10193955.
- ↑ Mitchell, Richard; Kumar, Vinay; Fausto, Nelson; Abbas, Abul K.; Aster, Jon (2011). Pocket Companion to Robbins & Cotran Pathologic Basis of Disease (8th ed.). Elsevier Saunders. pp. 254-5. ISBN 978-1416054542.
- ↑ URL: http://www.pathconsultddx.com/pathCon/diagnosis?pii=S1559-8675%2806%2970416-8. Accessed on: 28 March 2011.
- ↑ 10.0 10.1 10.2 10.3 Humphrey, Peter A; Dehner, Louis P; Pfeifer, John D (2008). The Washington Manual of Surgical Pathology (1st ed.). Lippincott Williams & Wilkins. pp. 282. ISBN 978-0781765275.
- ↑ URL: http://www.biology-online.org/dictionary/Heterologous. Accessed on: 1 October 2011.
- ↑ URL: http://www.thefreedictionary.com/palisaded. Accessed on: 2 February 2011.
- ↑ Coppes MJ, Haber DA, Grundy PE (September 1994). "Genetic events in the development of Wilms' tumor". N. Engl. J. Med. 331 (9): 586–90. doi:10.1056/NEJM199409013310906. PMID 8047084.
- ↑ Muir, TE.; Cheville, JC.; Lager, DJ. (Oct 2001). "Metanephric adenoma, nephrogenic rests, and Wilms' tumor: a histologic and immunophenotypic comparison.". Am J Surg Pathol 25 (10): 1290-6. PMID 11688464.
- ↑ Md Zin, R.; Murch, A.; Charles, A. (Jun 2011). "Pathology, genetics and cytogenetics of Wilms' tumour.". Pathology 43 (4): 302-12. doi:10.1097/PAT.0b013e3283463575. PMID 21516053.