Small cell carcinoma of the lung
| Small cell carcinoma of the lung | |
|---|---|
| Diagnosis in short | |
_by_core_needle_biopsy.jpg) Lung small cell carcinoma. H&E stain. | |
|
| |
| LM | stippled chromatin, high NC ratio with scant basophilic cytoplasm, typically small cells (~2x RBC diameter), +/-nuclear moulding, nuclei with smudgy appearance (Azzopardi phenomenon), necrosis, mitoses |
| Subtypes | large cell neuroendocrine carcinoma (LCNEC) |
| LM DDx | poorly differentiated adenocarcinoma of the lung, atypical carcinoid, lung carcinoid, metastatic small cell carcinoma, lymphoma, other small round blue cell tumours |
| Stains | chromogranin +ve, synaptophysin +ve, CD56 +ve, NSE +ve, TTF-1 +ve |
| Staging | lung cancer staging |
| Site | lung - see lung tumours |
|
| |
| Clinical history | smoking - usually a long history, heavy |
| Signs | +/-hemoptysis |
| Prevalence | not common |
| Radiology | lung mass, usu. central location |
| Prognosis | poor |
| Clin. DDx | other lung tumours (squamous cell carcinoma of the lung), metastatic tumours |
| Treatment | medical (chemotherapy) |
Small cell carcinoma of the lung, also small cell lung carcinoma (abbreviated SCLC)[1] is an aggressive malignant tumour of the lung. It is strongly associated with smoking.
Small cell carcinoma in general is dealt with in the small cell carcinoma article.
General
- Strong association with smoking.
- Typically treated with chemotherapy.
- Poor prognosis.
On a spectrum of lesions (benign to malignant):[1]
- Tumourlet.
- Carcinoid.
- Atypical carcinoid.
- Small cell carinoma/large cell neuroendocrine carcinoma (LCNEC).
Precursor lesion - uncommonly seen:
- Pulmonary neuroendocrine cell hyperplasia.[1]
Clinical:
- +/-Hemoptysis.
Gross
- Central location (close to large airways) - typical.
- Necrosis.
Images

Small cell carcinoma of the lung - centre of image. (WC/Rosen)
.jpg)
Microscopic
Features:
- Stippled chromatin.
- High NC ratio, scant basophilic cytoplasm.
- Typically small cells ~2x RBC diameter.
- +/-Nuclear moulding.
- Nuclei with a smudgy appearance (Azzopardi phenomenon).
- Necrosis.
- Mitoses.
Notes:
- There should be no nucleolus.
DDx:
- Poorly differentiated adenocarcinoma of the lung.
- Metastatic small cell carcinoma.
- Lymphoma.
- Atypical carcinoid.
- Basaloid squamous cell carcinoma of the lung.[2]
- Non-small cell carcinoma of the lung.
- Other small round blue cell tumours.
Subtypes
- Large cell neuroendocrine carcinoma (LCNEC).
Grading
As per CAP protocol (version 3.4.0.0):[3]
- G4 = undifferentiated - used for small cell carcinoma and large cell carcinoma.
Images
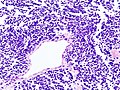
SCLC - low mag. (WC)
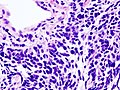
SCLC - high mag. (WC)
_by_core_needle_biopsy.jpg)
IHC
- Synaptophysin +ve.
- May be very weak.
- TTF-1 +ve
- CK7 -ve.[6]
- CK20 -ve.[6]
- Ki-67 ~80% (>50% proposed as criteria for large cell neuroendocrine carcinoma[7]).
- Useful for separating from atypical carcinoid and typical carcinoid.
Others:
Sign out
Lung, Left Lower Lobe, Core Biopsy: - SMALL CELL CARCINOMA.
Block letters
LOWER LOBE OF LUNG, LEFT, CORE BIOPSY: - SMALL CELL CARCINOMA.
Resection
Left Lower Lobe, Lobectomy:
- LARGE CELL NEUROENDOCRINE CARCINOMA.
-- Margins clear.
- Two lymph nodes NEGATIVE for malignancy (0/2).
- Please see synoptic report.
Comment:
The tumour stains as follows:
POSITIVE: CD56, synaptophysin, p63 (scattered).
NEGATIVE: chromogranin A, CK5/6, TTF-1, napsin A.
Micro
The sections show large cells epithelioid cells (~3-4x the size of a lymphocyte) with salt and pepper chromatin, scant basophilic cytoplasm, and focally streaming. Mitotic activity is brisk and multifocal zonal necrosis is present.
See also
References
- ↑ 1.0 1.1 1.2 Travis, WD. (Oct 2010). "Advances in neuroendocrine lung tumors.". Ann Oncol 21 Suppl 7: vii65-71. doi:10.1093/annonc/mdq380. PMID 20943645.
- ↑ Maleki, Z. (Mar 2011). "Diagnostic issues with cytopathologic interpretation of lung neoplasms displaying high-grade basaloid or neuroendocrine morphology.". Diagn Cytopathol 39 (3): 159-67. doi:10.1002/dc.21351. PMID 21319315.
- ↑ CAP Lung protocol. Version: 3.4.0.0. URL: http://www.cap.org/ShowProperty?nodePath=/UCMCon/Contribution%20Folders/WebContent/pdf/cp-lung-16protocol-3400.pdf. Accessed on: March 23, 2016.
- ↑ Misch, D.; Blum, T.; Boch, C.; Weiss, T.; Crolow, C.; Griff, S.; Mairinger, T.; Bauer, TT. et al. (Apr 2015). "Value of thyroid transcription factor (TTF)-1 for diagnosis and prognosis of patients with locally advanced or metastatic small cell lung cancer.". Diagn Pathol 10: 21. doi:10.1186/s13000-015-0250-z. PMID 25889870.
- ↑ Wu, M.; Szporn, AH.; Zhang, D.; Wasserman, P.; Gan, L.; Miller, L.; Burstein, DE. (Oct 2005). "Cytology applications of p63 and TTF-1 immunostaining in differential diagnosis of lung cancers.". Diagn Cytopathol 33 (4): 223-7. doi:10.1002/dc.20337. PMID 16138374.
- ↑ 6.0 6.1 Gyure, KA.; Morrison, AL. (Jun 2000). "Cytokeratin 7 and 20 expression in choroid plexus tumors: utility in differentiating these neoplasms from metastatic carcinomas.". Mod Pathol 13 (6): 638-43. doi:10.1038/modpathol.3880111. PMID 10874668.
- ↑ Liu, SZ.; Staats, PN.; Goicochea, L.; Alexiev, BA.; Shah, N.; Dixon, R.; Burke, AP. (2014). "Automated quantification of Ki-67 proliferative index of excised neuroendocrine tumors of the lung.". Diagn Pathol 9: 174. doi:10.1186/s13000-014-0174-z. PMID 25318848.
- ↑ Au, NH.; Gown, AM.; Cheang, M.; Huntsman, D.; Yorida, E.; Elliott, WM.; Flint, J.; English, J. et al. (Sep 2004). "P63 expression in lung carcinoma: a tissue microarray study of 408 cases.". Appl Immunohistochem Mol Morphol 12 (3): 240-7. PMID 15551738.