Radiation changes
| Radiation changes | |
|---|---|
| Diagnosis in short | |
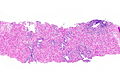
 Radiation changes. H&E stain. | |
|
| |
| LM | cytoplasmic vacuolation (usually abundant), enlarged nuclei - but usu. normal NC ratio, no nuclear membrane irregularies, chromatin "smudgy", +/-multinucleation, +/-fibrosis (chronic change), +/-edema (acute change) |
| LM DDx | pleomorphic tumours - esp. sarcomas, poorly differentiated carcinomas, drug/toxin effect, well-differentiated tumours in the background of radiation changes, "giant cell cystitis" |
| IHC | Ki-67 low, pankeratin -ve (usu.) |
| Site | pretty much anywhere |
|
| |
| Clinical history | history of radiation treatment/exposure - important for the diagnosis |
| Prognosis | benign |
| Clin. DDx | cancer recurrence, infection, new malignancy, post-surgical changes |
Radiation changes, also radiation effects, are seen occasionally by pathologists. They are usually a result of prior (radiation) treatments. The history is important in making this diagnosis.
General
- History of radiation treatment/exposure.
- Clinical symptoms dependent on site.
Gross
- +/-Erythema (early)
- +/-Fibrotic appearing tissue (late).
Microscopic
Features:[1]
- Cytoplasmic vacuolation - usually abundant.
- Nucleus:
- Enlarged nucleus - but normal NC ratio.
- No nuclear membrane irregularies.
- Chromatin: "smudgy".
- +/-Multinucleation.
- +/-Fibrosis (chronic change).
- +/-Edema (acute change).
Important note:
- The atypical cells are stromal cells; these survive the radiation. The epithelium is usually normal in the context of chronic changes.
- Pleomorphism is often suggestive of malignancy. Paradoxically, in the context of radiation, less pleomorphic (clonal-appearing) cells may be malignant!
DDx:
- Pleomorphic tumours.
- Well-differentiated carcinoma, e.g. postradiation prostatic carcinoma, may go unnoticed in the background of radiation-associated nuclear changes.
- Atypia associated with drugs.
- "Giant cell cystitis" - benign mesenchymal atypia with or without inflammation.
Images
Rectum

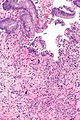
Radiation proctitis - low mag. (WC)
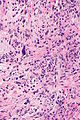
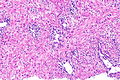
Radiation proctitis - intermed. mag. (WC)
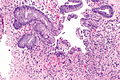
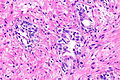
Radiation proctitis - high mag. (WC)

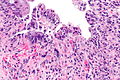
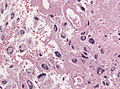
Radiation proctitis - very high mag. (WC)
Radiation proctitis - intermed. mag. (WC)

Radiation proctitis - high mag. (WC)
Radiation proctitis - high mag. (WC)







Prostate gland
Prostate with RC - low mag.
Prostate with RC - intermed. mag.
Prostate with RC - high mag.



Brain
Glioblastoma with RC (WC/jensflorian)

Radiation necrosis (WC/Tdvorak)

Radiation necrosis and gliosis (WC/Tdvorak)



IHC
- Pankeratin -ve.
- KI-67 low.
Sign out
RECTUM, BIOPSY: - SQUAMOUS MUCOSA WITH MARKED ACUTE INFLAMMATION AND REACTIVE CHANGES. - GRANULATION TISSUE. - LARGE ATYPICAL STROMAL CELLS AND FIBROSIS, COMPATIBLE WITH THE HISTORY OF RADIATION TREATMENT. - NEGATIVE FOR DYSPLASIA AND NEGATIVE FOR MALIGNANCY.
URINARY BLADDER, TRIGONE, BIOPSY: - INFLAMED UROTHELIAL MUCOSA WITH SQUAMOUS METAPLASIA, ULCERATION AND GRANULATION TISSUE FORMATION. - RADIATION CHANGES (STROMA). - NEGATIVE FOR DYSPLASIA AND NEGATIVE FOR MALIGNANCY.
Urinary bladder, biopsy: - Urothelial mucosa with evidence of ulceration (fibrin, necroinflammatory debris), mild stromal atypia and chronic inflammation, compatible with radiation cystitis - Negative for dysplasia - Negative for malignancy
Micro
Scattered rare large atypical cells with a preserved nucleus-to-cytoplasm ratio are present. Fibrosis is present.
See also
- Radiation colitis.
- Radiation esophagitis.
- Radiation changes in cervical cytology.
- Radiation changes of the endocervical epithelium.
- Radiation oncology.
- Endometrium post-ablation.